Complete blood count (CBC) - Platelets: Nursing
Complete blood count (CBC) - Platelets: Nursing
Watch later
Watch later
Notes
| PLATELETS | ||
| KEY POINTS | NOTES | |
| PHYSIOLOGY |
| |
| PATHOLOGY |
| |
| NURSING IMPLICATIONS |
| |
Transcript
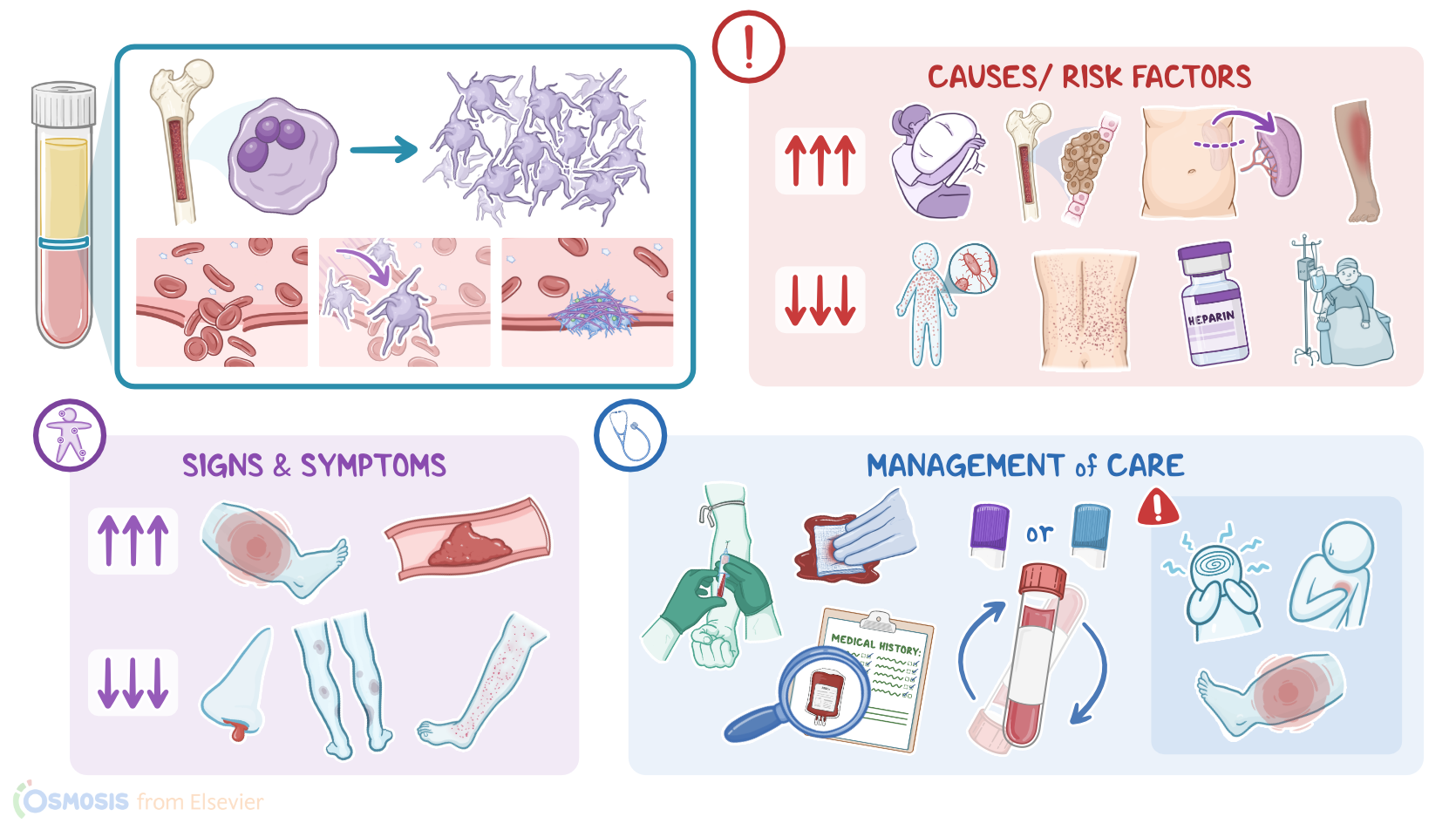
An older adult client is brought to the clinic because of a nosebleed that won’t stop. The client’s daughter states, “My dad has had frequent nosebleeds before, but it always stopped after a few hours.” On assessment, you notice pinpoint red spots on the client’s legs and trunk that don’t go away on pressure, and bruises on their arms and legs. Based on these findings, a complete blood count, or CBC, is ordered to check their platelet count. Now, platelets, also called thrombocytes, are cell fragments created in the bone marrow from cells called megakaryocytes. Plateletes are essential for beginning the process of coagulation. So, when a blood vessel is damaged, platelets stick to the inner surface of that blood vessel, aggregate together, and form a platelet plug to stop the bleeding. The lifespan of platelets is about 8 to 10 days. When they become old or damaged, they are removed by the spleen.
All right, the platelet count measures the number of platelets in the blood, and is usually measured as part of a CBC.The normal range for platelet count is from 150,000 to 450,000/μL. Now, there are some conditions that can alter the platelet count. When the platelet level is too high, it is called thrombocytosis. Trauma, inflammation, or blood loss can cause reactive thrombocytosis, where the platelet count becomes temporarily elevated, and then goes back to normal once the condition resolves. The platelet count can also temporarily increase after a splenectomy, because the platelets are not removed as fast as they are created. In contrast, conditions that can cause a sustained increase in platelets include certain myeloproliferative neoplasms, which are malignancies that cause the bone marrow to make too many platelets.
On the flipside, when the platelet level is too low, it is called thrombocytopenia. Now, sometimes the bone marrow doesn’t make enough platelets, which can happen in conditions like aplastic anemia, or with bone marrow depression from cytotoxic medications, like chemotherapy medications. On the other hand, healthy platelets can be destroyed due conditions like sepsis; autoimmune disorders like immune thrombocytopenia purpura; from a reaction to heparin, which is called heparin-induced thrombocytopenia; if platelets pool in an enlarged spleen; or even in clients with intravascular devices such as an intra-aortic balloon pump. Thrombocytopenia can also be the result of consumptive coagulopathies like disseminated intravascular coagulation, or DIC, where platelets are used faster than the body can make them. Lastly, thrombocytopenia can be idiopathic, meaning it occurs spontaneously and has no identified cause. This is referred to as idiopathic thrombocytopenic purpura.
Now, a client's platelet count is measured when a client is diagnosed with a condition that can alter the platelet count, or if there are signs and symptoms of high or low platelets. So, when platelets are increased, they can clump together and cause clots, or thrombosis, which can occlude blood vessels. When this happens in an extremity, clinical manifestations include swelling and pain from ischemia. Or the clot can travel and cause a venous thromboembolism. When clots form in other parts of the body, they can cause a heart attack or stroke. On the other hand, if platelets are low, the body will have difficulty making clots. So, clinical manifestations include easy bruising, petechiae, frequent nose bleeds, gastrointestinal bleeding, or even a brain hemorrhage. Okay, let’s look at the nursing implications for a client with an altered platelet count. Your priorities of care are to assist in restoring a normal platelet count and monitor for complications.