Contraception - Barrier methods: Nursing
1,046views
Contraception - Barrier methods: Nursing
Maternity Nursing
Maternity Nursing
Notes
| CONTRACEPTION - BARRIER METHODS | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
| PATHOPHYSIOLOGY |
| |
| PATIENT AND FAMILY TEACHING |
| |
Transcript
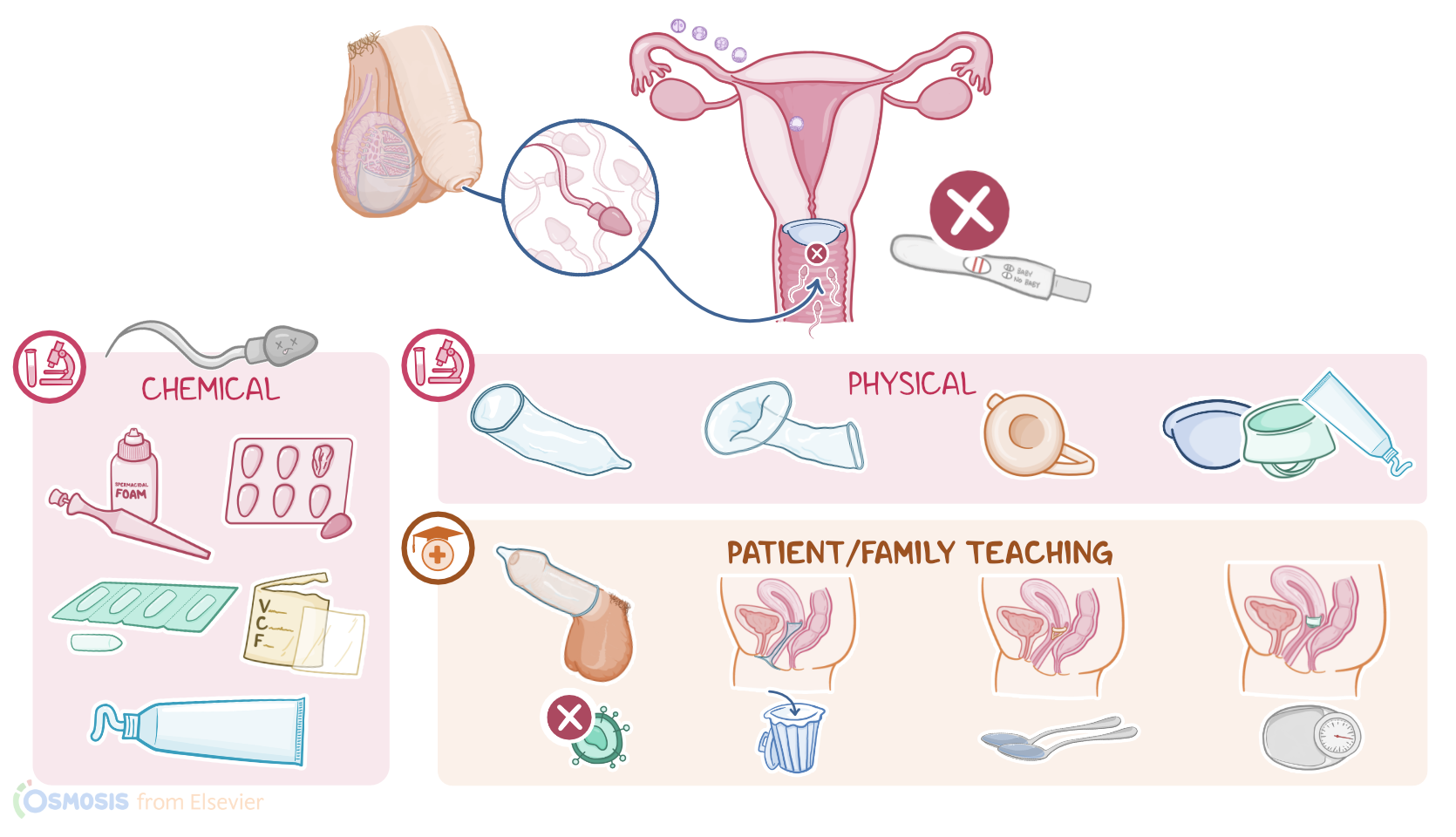
Barrier methods of contraception are reversible methods that can be used to prevent pregnancy. They get their name because they act as a “barrier” that prevents the sperm from getting into contact with the egg. They can be further classified as chemical or mechanical barriers, both of which prevent the sperm from entering the cervix.
Alright, now let’s quickly review the physiology of fertilization, starting with the ovaries, which are the paired female gonads. Each month, they release one mature egg, also called oocyte, which is the female gamete. After leaving the ovaries, this egg enters the fallopian tube and reaches the widest part of it, called the ampulla of the fallopian tube, where it can be fertilized by a sperm.
Sperm, on the other hand, is produced continuously by the testicles, and during intercourse, the penis releases it into the vagina. In order to reach the oocyte, sperm must cross the vagina, as well as the external cervical os, or opening, the endocervical canal, the internal cervical os, and the uterine cavity, to finally reach the fallopian tube, where one of them can finally fertilize the oocyte, so that a zygote is formed. The zygote then starts dividing and travels to the uterine cavity, where it can implant and develop into a fetus.
With this in mind, barrier contraceptives can act on several levels to prevent a sperm from meeting the oocyte. Let’s look at chemical barrier contraceptives first, namely spermicides. These are available as foams, foaming tablets, suppositories, vaginal films, creams, and gels. They contain chemical compounds like nonoxynol-9 or octoxynol that act like a surfactant, disrupting the sperm’s cell membrane, so the neck of the sperm detaches from the head, reducing mobility and causing cell death. So spermicides live up to their name by essentially killing sperm before they can enter the cervix. Overall, this method is about 80% effective as a contraceptive.
The advantage of spermicides is that they’re accessible, since they’re available without prescription and are inexpensive. They’re also easy to use, and they increase lubrication during intercourse. The downside is that effectiveness lasts less than an hour; they don’t protect from sexually transmitted disorders, or STDs, and they can can cause local irritation of the penis and vagina; and this mucosal inflammation can actually increase the risk of acquiring STDs. Some individuals might also find that spermicides interfere with the physical sensation during intercourse.
On the other hand, there are mechanical barrier contraceptives, which are placed over the penis or the cervix to prevent the sperm from passing through the endocervical canal and into the uterus. These include male and female condoms, and sponges; as well as the diaphragm or cervical cap.
Let’s start with the flagship of contraception, which are the male condoms. When used correctly, male condoms are up to 98% effective in preventing both pregnancy and STDs, including HIV. Advantages to male condoms are that they are readily available and cheap, and some clinics offer them for free. Condoms can be used together with spermicides, and some are even coated with spermicides. However, disadvantages include the risk of condom breakage; decreased efficacy if used incorrectly; and that some individuals may find them uncomfortable.
On the other hand, female condoms are 95% effective in preventing pregnancy. They are shaped like a small pouch with a flexible ring at each end. The smaller ring at the closed end is inserted into the vagina, while the larger ring remains outside the vagina. Female condoms provide protection from STDs, although they are less effective than male condoms for this purpose.
Next up, there are sponges which are round foam spermicide-containing discs that trap and kill sperm. So they’re actually a mix of mechanical and chemical barrier contraception. Efficiency ranges from 75% to 90%, depending on correct use. Disadvantages are that they don’t protect from STDs, and they can cause vaginal dryness and local irritation.