Diabetes mellitus (DM): Nursing process (ADPIE)
3,829views
Diabetes mellitus (DM): Nursing process (ADPIE)
SHRAVAM
SHRAVAM
Notes
| DIABETES MELLITUS | ||
| KEY POINTS | NOTES | |
| PATIENT REPORT |
| |
| PATHOPHYSIOLOGY |
| |
| DIAGNOSIS AND TREATMENT |
| |
| ASSESSMENT |
| |
| NURSING DIAGNOSES |
| |
| PLANNING |
| |
| IMPLEMENTATION |
| |
| EVALUATION |
| |
Transcript
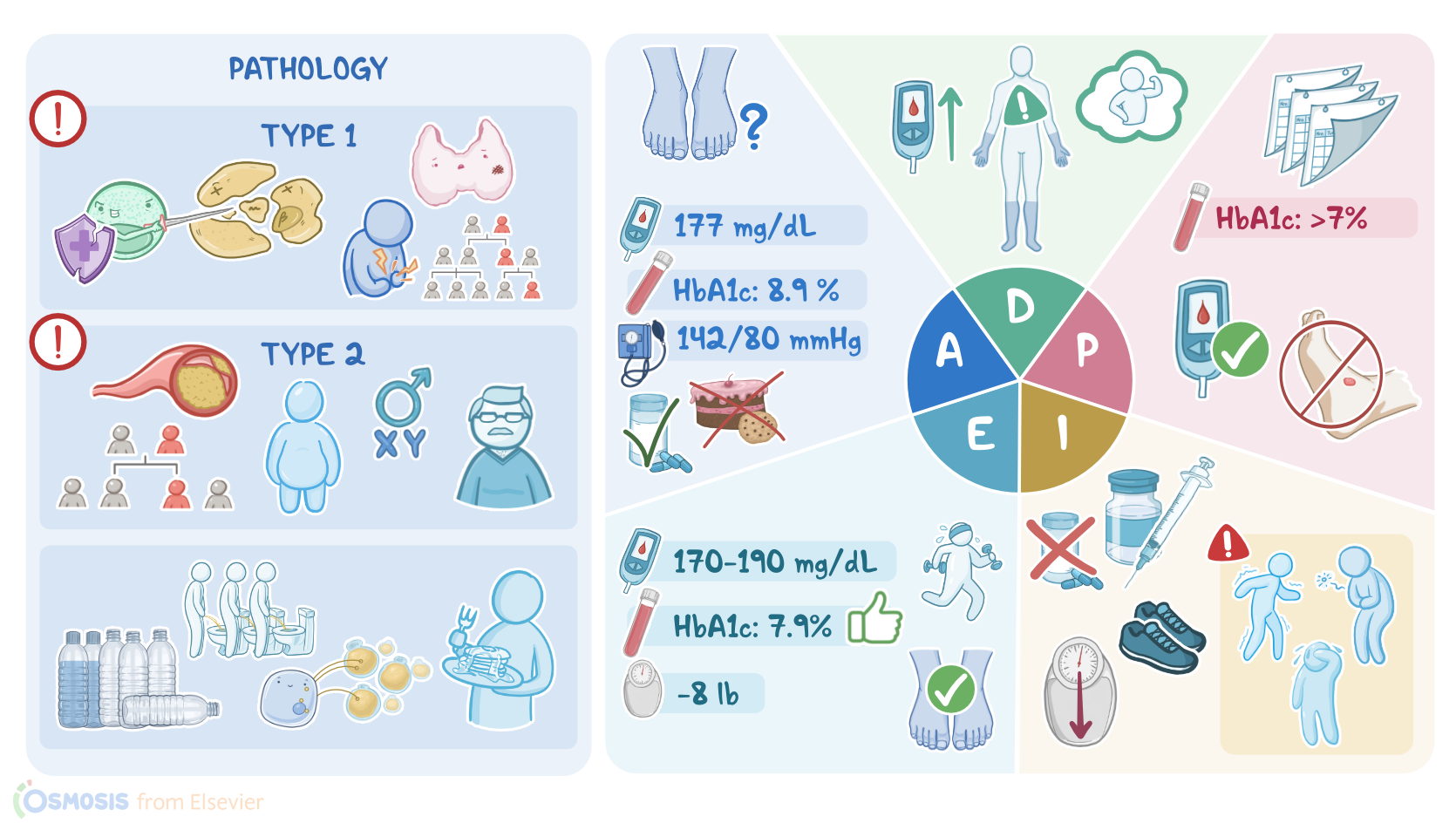
Harold Owl is a 63-year-old male client with a history of type 2 diabetes who is referred to the endocrinology clinic by his primary care provider for evaluation.
Mr. Owl takes the biguanide metformin and sulfonylurea glyburide to manage his diabetes, but his latest hemoglobin A1c, or HbA1c test, was 8.9% and he has recently developed numbness in his feet.
In diabetes mellitus, commonly just called diabetes, the body has trouble moving glucose from the blood into the tissue cells.
As a result, cells starve for energy despite having high blood glucose levels, which is called hyperglycemia.
Normally, high blood glucose stimulates the pancreatic beta cells to produce and secrete the hormone insulin, which in turn reduces blood glucose by stimulating the uptake of glucose into the cells. In diabetes, the blood glucose stays high because insulin’s function is impaired.
There are two main types of diabetes. In type 1 diabetes, there’s autoimmune destruction of the pancreatic beta cells, so they can’t produce and secrete insulin.
The exact cause of type 1 diabetes is unknown, but it’s thought to have a genetic and environmental component, and risk factors include personal or family history of type 1 diabetes, as well as celiac disease, and thyroid disease.
The onset is usually abrupt, generally appears before the age of 30, and is most often diagnosed during childhood or puberty.
On the other hand, in type 2 diabetes, the pancreas is able to produce and secrete insulin, but the tissue cells tend to be insulin resistant, meaning they are unable to respond well to insulin stimulation.
Type 2 diabetes is associated with risk factors, like male sex, increasing age, or having a first degree relative with type 2 diabetes, a body mass index or BMI over 25, a sedentary lifestyle, or a cardiovascular disease like hypertension.
With type 2 diabetes, the symptoms usually begin after the age of 45, and gradually worsen over a few months.
Classic symptoms of both type 1 and type 2 diabetes include polyuria, which means that individuals urinate frequently, which is associated with polydipsia, which means they are constantly thirsty and drink a lot of water.
Many clients also present with polyphagia, which is a fancy way to say they have a large appetite, and is associated with unexplained weight loss because tissue cells can’t uptake the glucose from food, so they instead use fatty acids from adipose tissue, called lipolysis.
Now, clients with type 1 diabetes are at risk for a serious acute complication called diabetic ketoacidosis, or DKA for short.
This occurs because, after lipolysis, the liver turns the fatty acids into ketone bodies, which increase the acidity of the blood.
As a result, clients can develop nausea, vomiting, dehydration, and a characteristic fruity smelling breath, as well as a deep and labored breathing called Kussmaul respirations.
Severe cases of DKA can also cause mental status changes and acute cerebral edema.
An acute complication that is much more common in type 2 diabetes is called hyperosmolar hyperglycemic state, or HHS, which is characterized by extreme hyperglycemia, along with increased urination.
This can cause severe dehydration, as well as nausea, vomiting, and mental status changes.
Alright, now over time, the hyperglycemia that occurs with uncontrolled diabetes can cause damage to the blood vessels, leading to long-term or chronic complications.
These include macrovascular complications due to damage to the larger blood vessels, resulting in peripheral vascular disease, myocardial infarction, and stroke.
Diabetes can also cause microvascular complications due to damage to the tiny blood vessels throughout the body.
In the kidneys, microvascular damage ultimately leads to diabetic nephropathy, which causes renal insufficiency and failure. In the eyes, microvascular damage can lead to diabetic retinopathy and can eventually cause blindness.
Diabetes can also affect the peripheral nerves, causing diabetic neuropathy, which is characterized by decreased sensation in the toes and fingers, sometimes called a stocking-glove distribution, as well as autonomic neuropathy, resulting in problems like delayed gastric emptying, called gastroparesis, as well as urinary retention, or neurogenic bladder, and erectile dysfunction in males.
Finally, a combination of microvascular damage and neuropathy can lead to the formation of diabetic foot ulcers, which can become infected easily, are slow to heal, and increase the risk of lower extremity amputation.
Diagnosing type 1 or type 2 diabetes is typically done by measuring blood glucose levels.
A random blood sample can be taken anytime, or very commonly, a fasting glucose sample where the person doesn’t eat or drink anything except water for 8 hours.
A fasting blood glucose level of 100-125 mg/dL is considered prediabetes, and if it's 126 mg/dL or higher on two separate occasions, the client has diabetes.
A non-fasting or random glucose test can be done at any time, with 200 mg/dL or higher being a red flag for diabetes.
Another test is called an oral glucose tolerance test, where a person is given glucose, and then blood samples are taken at time intervals to figure out how well it’s being cleared from the blood.
At the time interval of 2 hours later, a glucose level of 200 or above indicates diabetes.
Another type of test that can be done is the HbA1c test, which tests for the proportion of hemoglobin in red blood cells that has glucose stuck to it, called glycosylated hemoglobin.
Sources
- "Ackley and Ladwig’s Nursing Diagnosis Handbook: An Evidence-Based Guide to Planning Care, 13th edition" Mosby (2022)
- "Genetics of diabetes mellitus and diabetes complications" Nat Rev Nephrol (2020)
- "Harrison’s Principles of Internal Medicine, 21st edition" McGraw Hill / Medical (2022)
- "Definition, Classification and Diagnosis of Diabetes Mellitus" Exp Clin Endocrinol Diabetes (2019)
- "Diabetes, cardiovascular disease and the microcirculation" Cardiovasc Diabetol (2021)
- "Critical Care Nursing: Diagnosis and Management, 9th edition" Elsevier (2021)