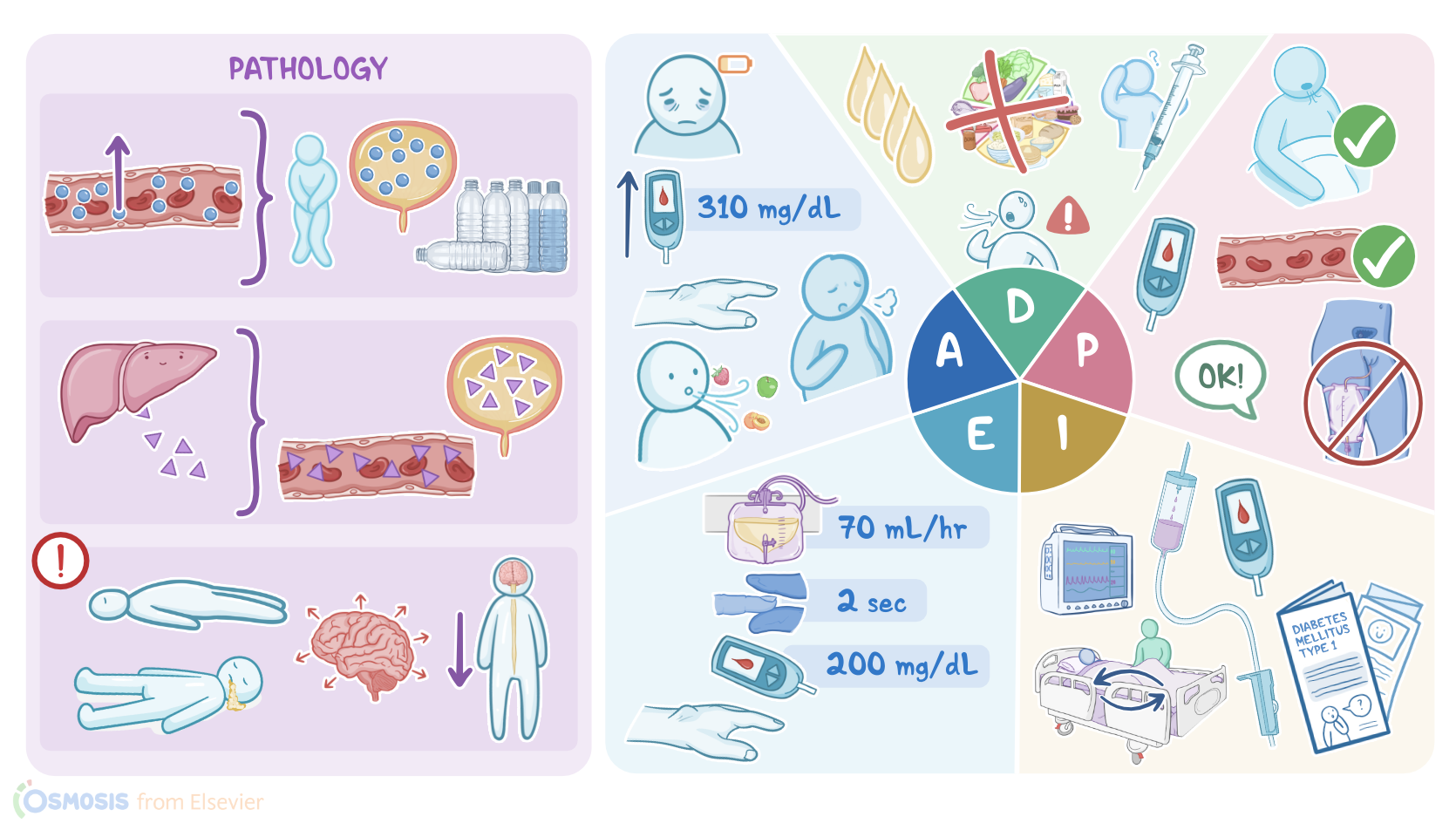
Diabetic ketoacidosis (DKA): Nursing process (ADPIE)
3,191views
Diabetic ketoacidosis (DKA): Nursing process (ADPIE)
Adults 2 Exam 1
Adults 2 Exam 1
Notes
| DIABETIC KETOACIDOSIS (DKA) | ||
| KEY POINTS | NOTES | |
| PATIENT REPORT |
| |
| PATHOPHYSIOLOGY |
| |
| ASSESSMENT |
| |
| NURSING DIAGNOSES |
| |
| PLANNING |
| |
| IMPLEMENTATION |
| |
| EVALUATION |
| |
Transcript
Content Reviewers
Juanita Perez is a 58-year-old female client with a history of Type 1 diabetes mellitus.
Mrs. Perez was brought to the Emergency Department (ED) late last night by her spouse, with complaints of severe lethargy, nausea, and a high blood glucose reading at home.
In the ED, she was found to have a blood glucose reading of 450 mg/dL.
She was immediately transferred to the Intensive Care Unit, or ICU with the diagnosis of diabetic ketoacidosis.
Diabetic ketoacidosis or DKA, is a serious complication of diabetes mellitus.
It occurs more commonly in type 1 vs type 2 DM because the cause is severe insulin deficiency.
When insulin levels are low, cells in the body can’t utilize glucose, so fat will be metabolized for energy instead.
The liver breaks down fat into Ketone bodies and as they build up in the blood, it causes a decrease in pH, leading to acidosis.
Risk factors for DKA include inadequate insulin administration, concurrent infection or illness, trauma, and injury.
DKA has a very sudden onset and it starts with a severely insufficient amount of circulating insulin.
If there’s not enough insulin, glucose is unable to enter cells to be used for energy.
The unused glucose builds up in the blood, causing hyperglycemia.
At this point the cells are really starving for glucose even though it’s plentiful in the blood.
So the liver releases glycogen and initiates glycogenolysis, where stored glycogen is broken down into glucose.
This is accompanied by the release of other counterregulatory hormones - cortisol, growth hormone, and catecholamines - which oppose the effects of insulin and initiate the breakdown of proteins to make additional glucose, a process called gluconeogenesis.
Blood glucose readings with DKA will typically be anywhere between 300-800 mg/dL.
As glucose levels increase, the renal threshold for glucose resorption is surpassed, which is why we’ll observe polyuria, glycosuria and dehydration caused by the loss of large volumes of urine laden with glucose.
As the liver breaks down fatty acids into ketone bodies for cells to use for energy, ketones build up in the blood and are excreted from the body with urine, resulting in ketonemia and ketonuria.
Unfortunately, ketones increase the acidity of the blood, which leads to the development of metabolic acidosis.
Acidosis is why we see Kussmaul respirations in clients with DKA.
To correct the acidosis, the body will automatically increase the respiratory rate in an attempt to blow off carbon dioxide and raise the blood pH.
Ketones are also exhaled out so the breath may have a “fruity scent.”
Acidosis also can lead to hyperkalemia, as cells exchange hydrogen ions with potassium.
On top of that, because insulin helps potassium enter the cell through the sodium-potassium pump, the lack of insulin means more potassium stays outside the cell, compounding the hyperkalemia.
Finally, if DKA persists, it can result in severe depression of the central nervous system, changes in the client’s level of consciousness, cerebral edema and eventually, coma.
Clients can decrease the risk of developing DKA by always taking their insulin as directed and monitoring their serum glucose often to make sure it stays within the desired range.
The right balance of physical activity and adherence to their diet plan is also essential. Because the body’s insulin needs change during illness and stress, clients need to monitor their blood glucose levels more closely during these times.
Any significant physical or emotional stressor can lead to hyperglycemia and DKA.
Now back to our client.
Upon going into your client’s room, you first wash your hands, then introduce yourself and verify your client’s identity.
You begin your assessment by asking Mrs. Perez how she is feeling.
She states she still feels very nauseous and tired.
You ask when she started feeling tired, and she states that yesterday morning she woke up feeling exhausted and not like herself, and that it continued throughout the day.
She goes on to say that yesterday, her blood glucose readings were a “little high”, with the lunch reading being 210 mg/dL and the dinner reading being 232 mg/dL.
You then ask if she has been taking her prescribed insulin as ordered.
She tells you that she recently lost her health insurance and because she can’t afford to refill her medications she’s been taking half the prescribed amount of insulin at each meal to try to make her current supply last.
You notice her respirations are very deep and appear to be labored when she talks, she tells you that it feels hard to breathe at times.
You smell that her breath has a sweet “fruity” odor.
You assess her heart and lungs, and determine that both are normal.
Key Takeaways
Diabetic ketoacidosis (DKA) is a serious condition usually seen in people with diabetes mellitus type 1. DKA happens when your body doesn't produce enough insulin to use glucose as an energy source, thus resolving to use fatty acids, and produce ketones. Ketones are poisonous, and they build up in your blood. If not treated, DKA can lead to coma or even death. Even though DKA usually happens to people with type 1 diabetes, it can also happen to people with type 2 diabetes. DKA presents with polydipsia, polyuria, vomiting, and dehydration. It can later progress to mental status changes, coma, and death if not treated on time.
Sources
- "Ackley and Ladwig’s Nursing Diagnosis Handbook: An Evidence-Based Guide to Planning Care, 13th edition" Mosby (2022)
- "Euglycemic diabetic ketoacidosis: The paradox of delayed correction of acidosis" Diabetes Metab Syndr (2023)
- "Harrison’s Principles of Internal Medicine, 21st edition" McGraw Hill / Medical (2022)
- "Diabetic Ketoacidosis" Emerg Med Clin North Am (2023)
- "Evaluation of Outcomes Following Hospital-Wide Implementation of a Subcutaneous Insulin Protocol for Diabetic Ketoacidosis" JAMA Netw Open (2022)
- "Critical Care Nursing: Diagnosis and Management, 9th edition" Elsevier (2021)