Epiglottitis: Nursing process (ADPIE)
Epiglottitis: Nursing process (ADPIE)
Nursing
Nursing
Notes
| EPIGLOTTITIS | ||
| KEY POINTS | NOTES | |
| PATIENT REPORT |
| |
| PATHOPHYSIOLOGY |
| |
| DIAGNOSIS AND TREATMENT |
| |
| ASSESSMENT |
| |
| NURSING DIAGNOSES |
| |
| PLANNING |
| |
| IMPLEMENTATION |
| |
| EVALUATION |
| |
Transcript
Content Reviewers
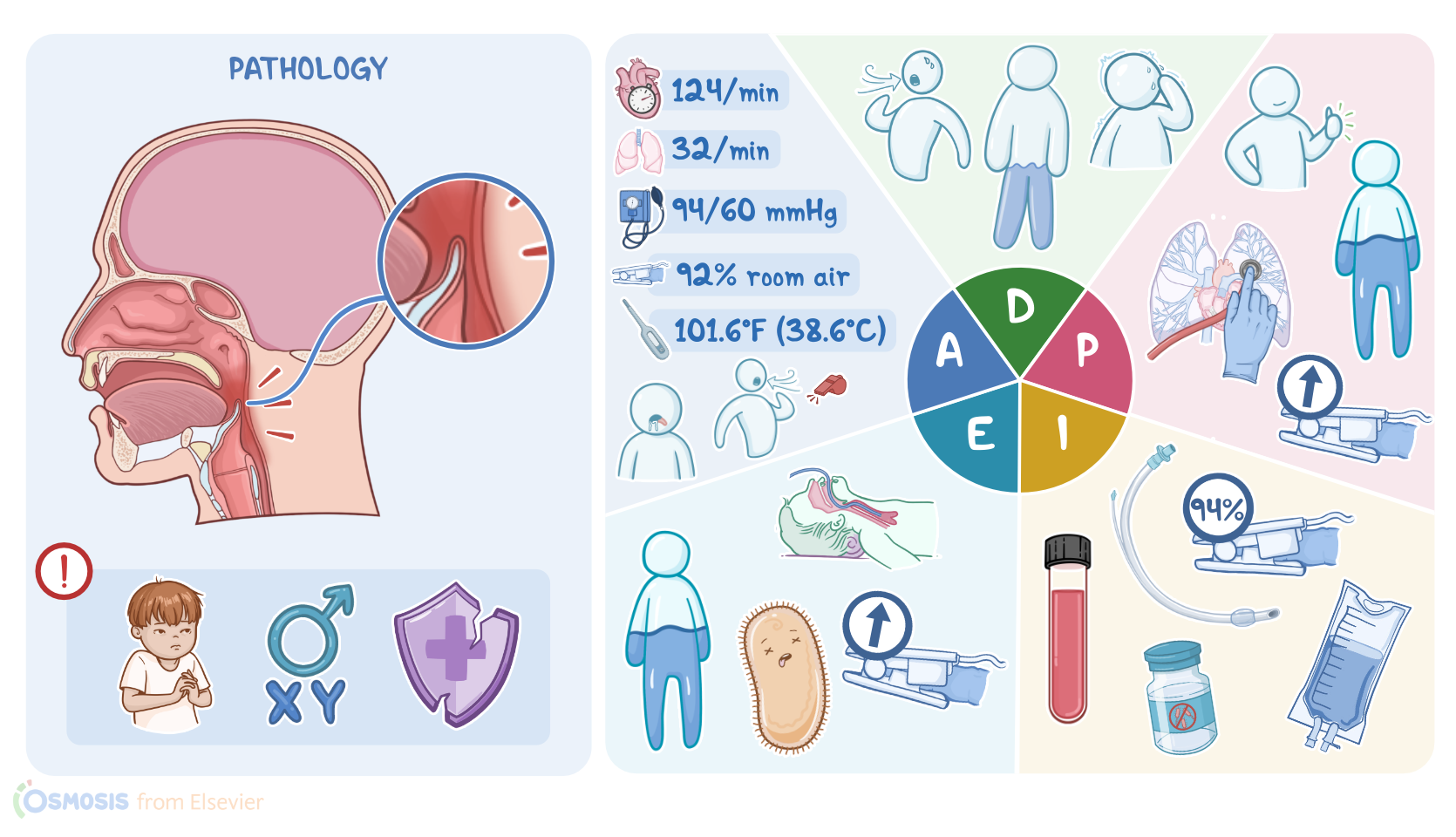
Eve Vu is a 5-year-old female who is brought to the emergency room, or ED, by her mother with reports of a sore throat and fever.
According to her mother, Eve has been irritable, refuses liquids, and when Eve started drooling, she brought her in as soon as she could.
Eve is triaged quickly for suspected epiglottitis.
Epiglottitis, also called supraglottitis, is inflammation of the epiglottis, which is a flap of cartilage located behind the tongue, and its surrounding tissues.
Epiglottitis typically occurs in children between 2 and 5 years of age, but can occur from infancy to adulthood.
Males are more at risk than females, and those who are immunocompromised are more at risk as well.
The most common causes used to be Haemophilus influenzae type b, but this has become less common thanks to an increase in childhood vaccination.
Streptococcus pneumoniae and Staphylococcus aureus are now the most common causes in the US.
Epiglottitis can also be caused by viral and fungal infections, or by non-infectious causes like smoke inhalation, hot foods or liquids, and foreign bodies.
In bacterial epiglottitis, the initial symptoms include sore throat and a sudden onset of high fever.
This can happen much quicker in children compared to adults.
When the epiglottis and nearby tissue become infected, inflammation and edema develops.
As the epiglottis swells up, it can fold backwards and act like a ball valve that obstructs the airways during inhalation.
The swelling of the nearby tissue makes matters worse by narrowing the airways.
In children, this will lead to the 3 Ds; Distress or anxiety, Dysphagia, or difficulty swallowing, and Drooling due to the inability to swallow.
Airway obstruction can also cause turbulent airflow resulting in an inspiratory stridor which sounds like a high pitched whistling.
The voice also becomes muffled so it sounds like they have a hot potato in their mouth when they speak.
The work of breathing is increased so you’ll often see suprasternal and substernal retractions.
To breathe easier, children will often sit upright and lean forward in a tripod position, with the chin thrust out, mouth open, and tongue protruding to help keep the airway open.
Severe airway obstruction can lead to hypoxia, hypercapnia, and acidosis, followed by loss of consciousness and death.
The diagnosis of epiglottitis is based on the client’s history and physical examination.
Direct visualization can show inflammation of the throat and a large, cherry red epiglottis, but it should be avoided in children and anxious clients due to the risk of triggering laryngeal spasms that could worsen the obstruction.
Other anxiety-producing procedures such as IV placement, phlebotomy, supine positioning, and oral examination should also be postponed until the airway is secured.
A lateral neck x-ray will show an enlarged epiglottis that looks like a thumbprint.
Throat cultures obtained during intubation and blood cultures can confirm the organism and help make sure the right treatment is prescribed.
Treatment for epiglottitis is first focused on airway management, and once the airway is secured, antibiotics can be used to treat the infection.
Prevention measures include immunization against Hib beginning at 2 months of age to help prevent epiglottitis and other serious infections.
Okay, now that we’ve reviewed epiglottitis, let’s get back to assess our client, Eve.
You wash your hands, introduce yourself, and confirm Eve’s identity.
Sources
- "Ackley and Ladwig’s Nursing Diagnosis Handbook: An Evidence-Based Guide to Planning Care, 13th edition" Mosby (2022)
- "Medical Management of Epiglottitis" Anesth Prog (2020)
- "50 Years Ago in The Journal of Pediatrics: Acute Epiglottitis: To Trach or Not to Trach" J Pediatr (2023)
- "Epiglottitis with abscess as a source of airway obstruction" Visual Journal of Emergency Medicine (2023)
- "Harrison’s Principles of Internal Medicine, 21st edition" McGraw Hill / Medical (2022)
- "Intubation decision criteria in adult epiglottitis" Eur Ann Otorhinolaryngol Head Neck Dis (2021)