Eye injury: Nursing process (ADPIE)
Client Report0:00–1:01
Kevin Stackhouse is a 25 year old male construction worker who presents to the emergency department or ED after sustaining an injury to his eye when a panel of glass shattered during installation.
Mr. Stackhouse reports he experienced sharp pain followed by vision loss in his right eye.
Upon arrival to the ED, he was found to have swelling and lacerations in his periorbital area, as well as pain and decreased eye movement.
The on-call ophthalmologist performs a slit lamp examination and fundoscopy, which reveals two small glass fragments present in the eye, along with a corneal laceration.
Mr. Stackhouse is given a tetanus booster and is taken to the operating room or OR for surgical removal of the fragments and repair of the corneal laceration.
Pathology1:01–6:01
Penetrting eye injuries occur when the eye is pierced by a sharp object such as pencils, screwdrivers, nails, knives, as well as high velocity flying fragments like those from fireworks and other explosions.
Now, there are some factors that may put the client at risk for penetrating eye injuries. Modifiable risk factors include occupations that have exposure to sharp objects, such as construction workers, mechanics, or being in the military.
On the other hand, a non-modifiable risk factor is male gender, and that's probably because males are more likely to have high-risk occupations.
Another non-modifiable risk factor is age. In particular, children are at increased risk for penetrating eye injuries, since they can be careless or less coordinated when playing.
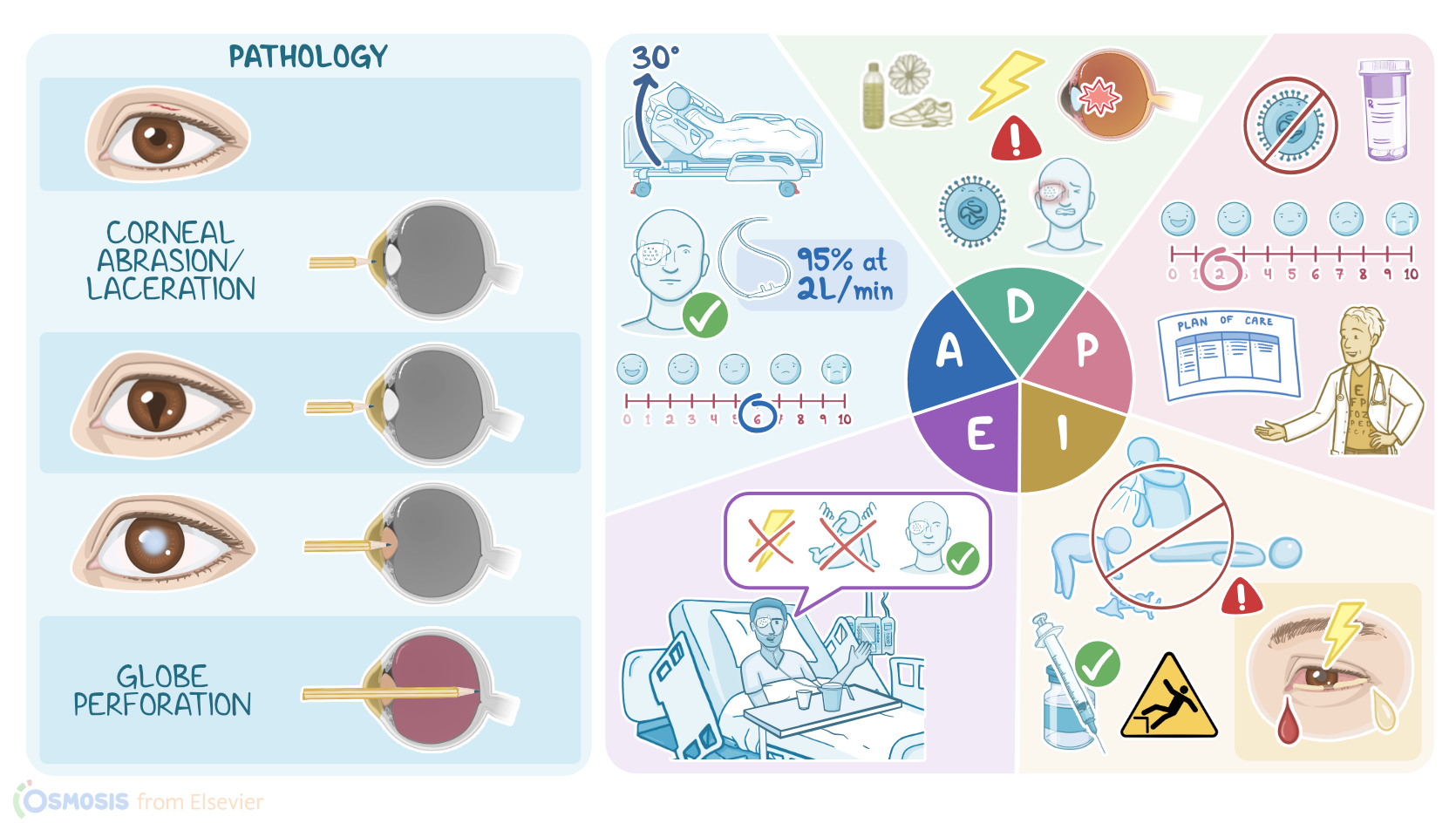
Now the extent of the penetrating eye injury depends on its depth. So first, there's eyelid laceration, which is a skin cut on the eyelid.
Next, if the penetrating object makes it to the cornea, it may result in corneal abrasion, which is a superficial scratch, or a corneal laceration, which is a deeper cut.
Behind the iris is the lens, which may be disrupted, leading to a traumatic cataract where the lens becomes opaque and cloudy.
In severe cases, the object may cause globe perforation, which is when the sharp object penetrates the eyeball to the other side.
Clients with penetrating eye injury are at risk of complications like traumatic glaucoma, where part of the trabecular meshwork becomes blocked, preventing the normal outflow of the aqueous humor and ultimately increasing the intraocular pressure.
The penetrating object may also lead to vitreous hemorrhage, where blood leaks into the vitreous space. This may ultimately lead to retinal detachment, where the retina pulls away from the underlying layers in the eye.
If vitreous hemorrhage or retinal detachment occur, the client may see floaters or shadows. Now, one of the main complications of penetrating eye injury is endophthalmitis, which is a serious bacterial infection within the eye due to bacteria that manage to enter the eye through the wound.
Finally, penetrating eye injury can also result in permanent visual impairment or even complete vision loss. When penetrating eye injury is suspected, based on history and physical exam, the first thing to do is to seek emergency care.
The main diagnostic studies used include slit lamp examination and fundoscopy, which look for injuries in foreign bodies within the eye.
In addition, fluorescence staining can be used to stain the cornea, and this allows detection of damage like corneal abrasion.
In addition, tonometry can be performed to measure the intraocular pressure to check for glaucoma. Finally, imaging studies like ultrasound, X-ray, and CT scan can be used to look for intraocular foreign bodies and any associated injuries to nearby structures like orbit fractures.
Keep in mind that MRI is contraindicated if the penetrating injury is suspected to be due to a metallic object, as its use may cause the object to move inside the eye, causing further damage.
If there's a foreign object inside the eye, the client shouldn't try to remove it. Instead, the eye should be protected from further damage using a plastic or metal shield.
In addition, no pressure should be applied to the eye, and the client should be instructed not to cough, sneeze, or bend to prevent the extrusion of eye contents to the outside.
The client should be given IV antibiotic prophylaxis with vancomycin and either ceftazidine or ciprofloxacin. Finally, some clients may need surgery to remove any foreign bodies and repair the damage.
You begin your assessment as you receive Mr. Stackhouse from the Transferring Post anesthesia care unit or PACU nurse who informs you that all glass fragments were successfully removed and the corneal laceration was repaired.
Assessment6:01–7:17
Mr. Stackhouse is groggy, but oriented to person, place, and time.
You elevate the head of the bed 30 degrees and assess his vital signs, which are temperature 98.5 °F or 36.9 °C. Heart rate 65 BPM and regular, respiratory rate 18 breaths per minute with clear lung sounds bilaterally.
BP 120/78 millimeters of mercury. Oxygen saturation, 95% with oxygen at 2 L per minute via nasal cannula, and his pain is 6 out of 10 in his right eye.
There is a cover in place over his eye consisting of a sterile patch and a protective shield. The dressing is clean, dry and intact.
You document your assessment findings and continue to monitor him for any changes. Now you establish your nursing diagnoses for Mister Stackhouse, which include disturbed visual sensory perception related to surgical intervention and patching of the eye, acute pain related to trauma to the globe and periorbital area, risk for infection related to the impaired integrity of the ocular tissue, and risk for injury related to visual impairment.
Diagnosis7:17–7:41
Planning7:41–8:12
Next, you collaborate with Mr. Stackhouse and the ophthalmologist to develop goals for his plan of care.
One hour after medication administration, his pain level will be at his stated tolerance level of 2 out of 10. Up until the time of discharge, he will remain free from infection and injury.
And after discharge, Mr. Stackhouse will demonstrate the ability to adapt to any remaining visual sensory perception disturbances.
Implementation8:12–9:56
Now you are ready to implement the plan of care. First, you administer the ordered analgesic and IV antibiotic.
You explain how this will help make him more comfortable and help prevent an infection from developing in his eye, and you let him know that you will be checking on him frequently to monitor his pain and signs of a developing infection.
Next, you institute fall precautions, place needed items within reach and stress the need to call for assistance for any needs he may have.
After Mr. Stackhouse is more alert, you provide him with information he will need to protect his eye and remain free from injury after discharge.
You explained to Mister Stackhouse that he must leave the protective eye cover in place, making sure to avoid applying pressure to the affected eye.
Next, you review safety measures to prevent falls and other injuries at home and advise him to call his ophthalmologist if he develops problems, such as a feeling of pressure or increased pain in the eye, or if he notices bleeding or other discharge from the eye.
You remind him that he will be following up with his ophthalmologist 3 days after he is discharged home for continued support of healing and assessment of his visual acuity.
During your shift, you continue to monitor Mr. Stackhouse and we'll notify the surgeon if he experiences any sudden changes to his current condition.
OK, it's time to evaluate to see how Mister Stackhouse is progressing. His pain rating is currently 0 out of 10.
Evaluation9:56–10:33
His vital signs are stable, and his surgical dressing is clean, dry, and intact. Mr.
Stackhouse has not experienced a fall during your shift, and he has explained in his own words, the safety measures needed to protect his eye and to prevent falls and other injuries while his eye is healing.
You continue to evaluate the effectiveness of your interventions and adjust Mr. Stackhouse's plan of care as needed.
Summary10:33–11:24
All right, as a quick recap, your client, Kevin Stackhouse, is a 25 year old male construction worker who presented to the ED after glass fragments embedded in his eye, causing him to experience vision loss in his right eye.
After the glass fragments were removed surgically, your assessments identified problems, and you developed nursing diagnoses to address them, including disturbed visual sensory perception, pain, risk for infection, and risk for injury.
The goals you planned focused on pain management, infection prevention, and safety. Along with the healthcare team, you work to implement interventions to achieve the goals of the plan of care.
Throughout your shift, you will continue to evaluate and revise your plan of care as needed.
| EYE INJURY | ||
| KEY POINTS | NOTES | |
| PATIENT REPORT |
| |
| PATHOPHYSIOLOGY |
| |
| DIAGNOSIS AND TREATMENT |
| |
| ASSESSMENT |
| |
| NURSING DIAGNOSES |
| |
| PLANNING |
| |
| IMPLEMENTATION |
| |
| EVALUATION |
| |
- "Ackley and Ladwig’s Nursing Diagnosis Handbook: An Evidence-Based Guide to Planning Care, 13th edition" Mosby (2022)
- "Photophobia: shared pathophysiology underlying dry eye disease, migraine and traumatic brain injury leading to central neuroplasticity of the trigeminothalamic pathway" Br J Ophthalmol (2021)
- "Chemical eye injury: pathophysiology, assessment and management" Eye (Lond) (2020)
- "Penetrating eye injury by dart" Int J Legal Med (2021)
- "Eye injuries: Understanding ocular trauma" Aust J Gen Pract (2022)
- "Harrison’s Principles of Internal Medicine, 21st edition" McGraw Hill / Medical (2022)
- "Immune responses to injury and their links to eye disease" Transl Res (2021)
- "Corneal wound healing" Exp Eye Res (2020)
No notes for this video yet
Try adding a note below