Frostbite: Nursing process (ADPIE)
Frostbite: Nursing process (ADPIE)
Medical Surgical
Medical Surgical
Notes
| FROSTBITE | ||
| KEY POINTS | NOTES | |
| PATIENT REPORT |
| |
| PATHOPHYSIOLOGY |
| |
| DIAGNOSIS AND TREATMENT |
| |
| ASSESSMENT |
| |
| NURSING DIAGNOSES |
| |
| PLANNING |
| |
| IMPLEMENTATION |
| |
| EVALUATION |
| |
Transcript
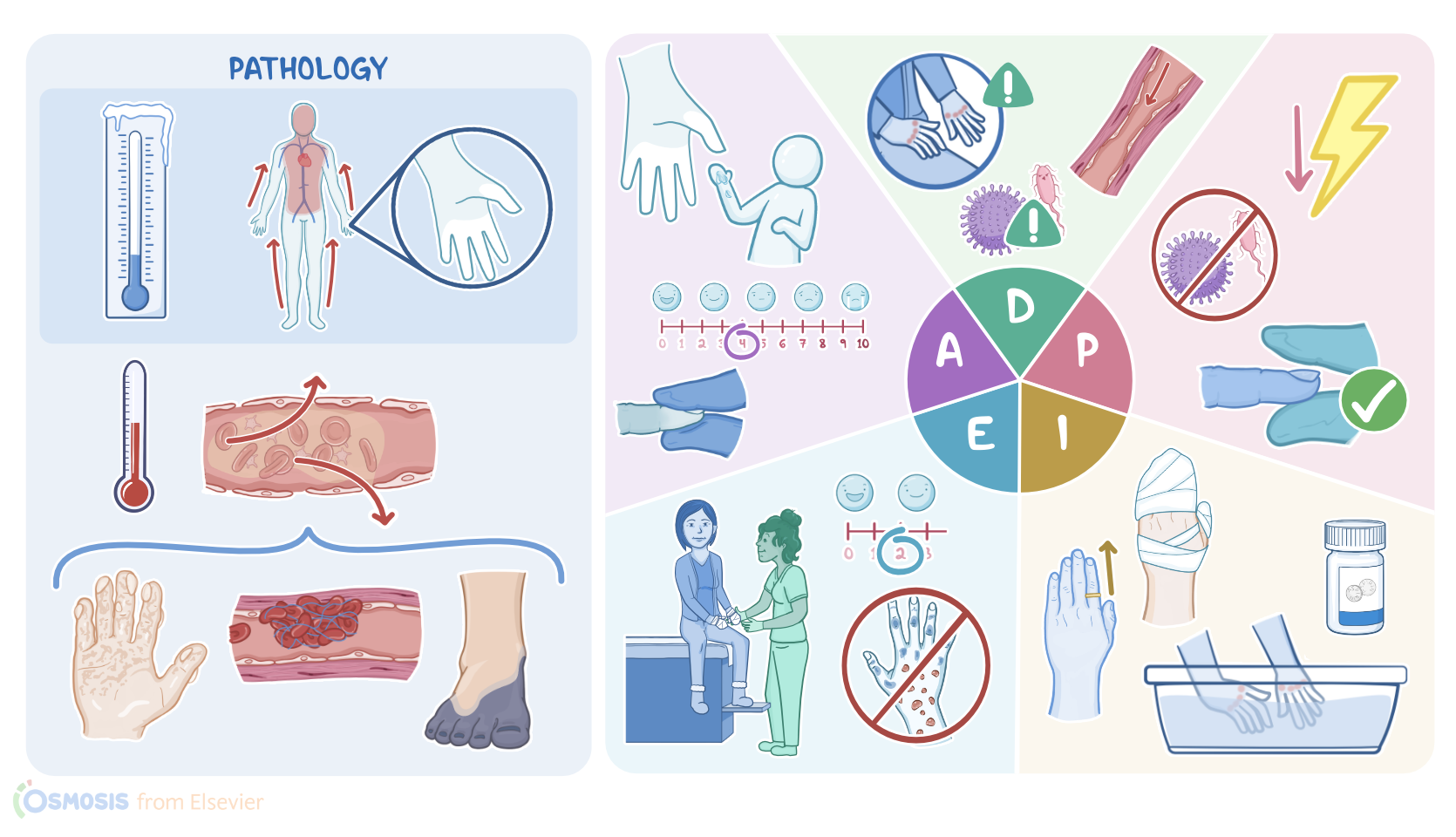
Christine Lee is a 46-year-old woman who presents to your emergency department after changing a flat tire in the cold with her bare hands. The temperature outside was around 29 degrees F, or minus 1.7 degrees C. Ms. Lee is concerned about her hands and fingers. She says that her fingers feel numb and tingly. Her fingertips are pale and cool, while her knuckles are red, warm, and swollen. The physician diagnoses Ms. Lee with frostbite.
Frostbite is defined as a severe localized injury that occurs when a part of the body such as hands, feet, and face, is exposed to temperatures below 31 degrees F or minus 0.5 degrees C. It typically occurs within 30 minutes where the skin is exposed to low temperatures and windy weather.
Normally, our body responds to low temperatures by constricting small blood vessels close to the skin. This way, it prevents loss of heat by shifting the warm blood from the extremities to internal organs. As a result, the exposed skin becomes pale, cold, and numb; and a person starts to experience a tingling and aching sensation. Next, low temperatures cause intracellular and extracellular fluids to freeze and form small ice crystals that give the tissue a firm, solid feel. Furthermore, these ice crystals directly damage the surrounding tissue and vascular endothelial cells. And, if the exposure to low temperatures continues, blood vessels can lose their vascular tone, eventually causing the pooling of blood and changing the skin color from pale to purplish.
Now, when the affected part of the body is rewarmed, the blood flow is restored and reperfusion injury occurs. In reperfusion injury, damaged blood vessels leak fluid into surrounding tissue, eventually causing edema. At this point, the skin develops a blotchy appearance. The blotchy skin can be followed by fluid-filled blisters, which most commonly occurs in the next 24-48 hours. At the same time, damaged blood vessels initiate platelet aggregation, eventually causing thrombosis and further reduction of the blood flow. On the flip side, damaged tissue stimulates leukocytes to produce cytokines, thereby inducing inflammation and further destruction of the affected part of the body. In severe cases, tissue destruction can progress to skin necrosis, which typically presents as a blue-gray discoloration of the skin.
So, the diagnosis of frostbite is based on the detection of these changes on the skin during a physical exam. Additionally, we can check whether or not the person has peripheral pulses in the affected extremity. In some cases the pulse may not be palpable, so pulses should be checked using Doppler ultrasound.
Now, there are some factors that can put a person at risk for frostbite and they can be subdivided into several groups. The first group includes environmental factors like low temperature, the duration of exposure, high altitude, wind, and wet clothes. Next, we have individual risk factors, such as age, gender, and race. For example, infants and the elderly have limited thermoregulation abilities so they have a harder time producing and retaining body heat. The third group includes health risk factors, such as exhaustion and dehydration, which can further decrease the ability of the body to adapt to low temperatures. Other important health risk factors include previous frostbite or cold injuries, and medical conditions associated with poor circulation, such as diabetes. Additionally, the use of vasoconstrictive substances, such as beta blockers and nicotine from smoking, increases the risk of freezing because they narrow small blood vessels in the hands and feet. Finally, we have behavioral risk factors, such as alcohol, and substance abuse, which can all lead to an altered mental status that prevents the person from seeking shelter.
Now, it’s important to note that frostbite can lead to some serious complications. First, it can progress to hypothermia, which is a condition when a person’s core body temperature drops below 95 degrees F or 35 degrees C. Next, damaged skin offers little protection against pathogens so there’s an increased risk of infection. Moreover, bacterial infection can progress to gangrene, which is a condition associated with severe tissue destruction that might require the amputation of the affected extremity. On rare occasions, the bacteria called Clostridium tetani can enter the body and cause severe generalized muscle contractions, often referred to as tetanus.
Treatment of frostbite requires rewarming of the affected part using warm water that ranges from 98.6 to 102.2 degrees F, or 37 to 39 degrees C. Additionally, clients should take nonsteroidal anti-inflammatory drugs to relieve pain; and thrombolytics to reduce the risk of thrombosis and reperfusion injury. Finally, severe frostbites associated with necrosis require wound care and removal of dead tissue.
Sources
- "Ackley and Ladwig’s Nursing Diagnosis Handbook: An Evidence-Based Guide to Planning Care, 13th edition" Mosby (2022)
- "Frostbite: Current status and advancements in therapeutics" J Therm Biol (2020)
- "Interventions for frostbite injuries" Cochrane Database Syst Rev (2020)
- "Harrison’s Principles of Internal Medicine, 21st edition" McGraw Hill / Medical (2022)
- "Long-Term Sequelae of Frostbite-A Scoping Review" Int J Environ Res Public Health (2021)
- "Diagnosis and Treatment of Frostbite" N Engl J Med (2022)
- "Practical Review of the Current Management of Frostbite Injuries" Plast Reconstr Surg Glob Open (2022)