Gestational trophoblastic disease: Nursing
Gestational trophoblastic disease: Nursing
Medical Surgical
Medical Surgical
Notes
| GESTATIONAL TROPHOBLASTIC DISEASE | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
| CAUSES AND RISK FACTORS |
| |
| PATHOPHYSIOLOGY |
| |
| SIGNS AND SYMPTOMS |
| |
| DIAGNOSIS |
| |
| TREATMENT |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
Transcript
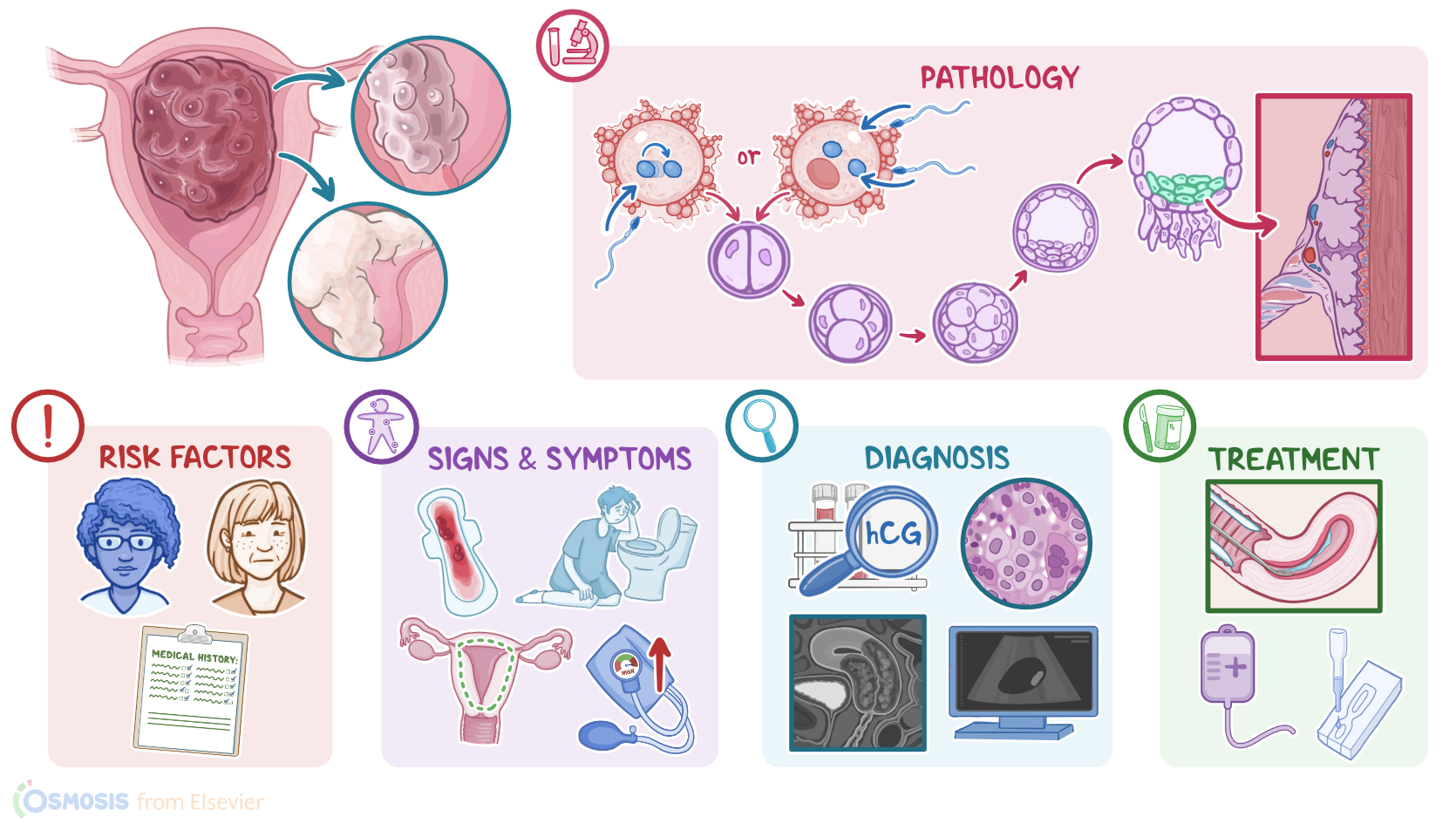
Gestational trophoblastic disease includes both benign and malignant proliferations of placental cells. At the benign end of the spectrum, there’s hydatidiform mole, also called molar pregnancy; while at the malignant end, there’s gestational trophoblastic neoplasia, which includes choriocarcinoma and trophoblastic tumors. Now, let’s quickly review the physiology of fertilization. Normally, at fertilization, a single female gamete, or the egg fuses with a single male gamete, called the sperm. Both the egg and the sperm normally have 23 chromosomes each, so half the set of human chromosomes. When combined, they give rise to a new organism, called the zygote, with 46 chromosomes. Now, the zygote undergoes repeated mitosis to produce more cells, which are grouped into the inner and the outer layer. The inner cells develop to become the embryo, whereas the outer cells, called the trophoblasts, form the embryonic part of the placenta, called the chorion, and its projections, known as chorionic villi. The chorion produces beta human chorionic gonadotropin, or beta-hCG for short, which is a hormone that helps in maintaining the pregnancy. Now, gestational trophoblastic disease is the result of genetic abnormalities that occur during fertilization, leading to abnormal proliferation of trophoblastic tissue.
Risk factors include age extremes, like younger than 16, or older than 45; a personal history of gestational trophoblastic disease; and Asian race. All right let’s switch gears and talk about pathology. Hydatidiform mole develops when a chromosomally empty egg fuses with a normal sperm. The sperm's genetic material duplicates to form 46 chromosomes. Because there are only paternal chromosomes, the mole develops into a mass of cells without any fetal parts or placenta. This is called a complete mole. An incomplete mole, on the other hand, appears when a normal egg is fertilized by two sperm, which develops 69 chromosomes. In both cases there is a proliferation and edema of the chorionic villi, which form grape-like structures that rapidly fill the uterus. These structures also secrete an excessive amount of hCG. Now, a hydatidiform mole is considered premalignant, which means it sometimes develops into a malignant invasive mole that can spread to the uterus and even metastasize. Additionally, choriocarcinoma can arise from a hydatidiform mole or independently, and is highly malignant. When it comes to complications these include preeclampsia, hemorrhage, uterine infections, sepsis, and metastasis.
Clinical manifestations of gestational trophoblastic disease include a uterus that is often larger than expected for gestational age, as well as vaginal bleeding, which can range from brown to bright red spotting to profuse hemorrhage; and grapelike molar vesicles might be expelled vaginally. Other findings include excessive nausea and vomiting, also known as hyperemesis gravidarum, and high blood pressure. Finally, fetal heart tones are absent. Now, the diagnosis of gestational trophoblastic disease starts with the client’s history and physical examination, followed by diagnostic blood tests, such as hCG levels, which are typically higher than expected. This is usually followed by an ultrasound that shows a characteristic snowstorm appearance caused by a collection of abnormal gestational sacs. For a definitive diagnosis, histopathologic evaluation is required. Additional imaging studies, like an x-ray, CT, and MRI can also be done to look for evidence of malignancy. Treatment for gestational trophoblastic disease is to remove the trophoblastic tissue from the uterus, usually through suction curettage. Continuous follow-up with hCG values should also be done after the procedure to detect malignant changes of any remaining trophoblastic tissue. Malignant tumors might require additional treatment, such as chemotherapy.
Let’s discuss the care you’ll be providing for the client with a complete hydatidiform mole. Priority goals of nursing care include addressing symptoms, assisting with surgical intervention, and providing emotional support. Begin by assessing your client’s bleeding, blood pressure, and degree of hyperemesis. Administer the prescribed IV fluids to maintain circulating volume. Then, administer the prescribed antihypertensive and antiemetic medications. Next, assist with evacuation of the uterine contents. Add oxytocin to the IV at the beginning of the procedure to control bleeding, as ordered. After the procedure, assess for post treatment pain, and administer the prescribed analgesics, as needed. If your client is RhD-negative, be sure to administer Rho (D) immune globulin within 72 hours after the procedure to prevent isoimmunization. Finally, provide emotional support for your client, may can be experiencing emotions like powerlessness, fear, and grief, due to their pregnancy loss. Assess their support system and refer them to local community resources, as needed.