Hemolytic disease of the fetus and newborn: Nursing
Hemolytic disease of the fetus and newborn: Nursing
Acute Final
Acute Final
Notes
| HEMOLYTIC DISEASE OF THE FETUS AND NEWBORN | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
| CAUSES AND RISK FACTORS |
| |
| PATHOPHYSIOLOGY |
| |
| SIGNS AND SYMPTOMS |
| |
| DIAGNOSIS |
| |
| TREATMENT |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
Transcript
Hemolytic disease of the fetus and newborn, also called erythroblastosis fetalis, is an immune-mediated condition in which the red blood cells of the fetus or newborn are hemolyzed, or destroyed by the mother’s antibodies. Let’s start by looking at the physiology of blood groups. The most common blood group classification is based on the ABO and the Rh system. These systems are based on the presence or absence of certain glycoproteins on the surface of red blood cells. The ABO system relies on the presence or absence of type A and B glycoproteins on RBCs. So people with the A blood type have type A glycoproteins; people with B blood type have type B glycoproteins; people with type AB, intuitively, have both; and people with the O blood type have neither type of glycoproteins on their RBCs. The immune system produces antibodies against the glycoproteins that are missing from the surface of the individual’s erythrocyte. That’s why people with type A blood have antibodies to type B blood, and those with type B blood have antibodies to type A blood. People with blood type AB don’t have antibodies to type A or type B blood; whereas people with type O blood have antibodies to both A and B glycoproteins.
Next, the Rh classification looks at whether or not the Rhesus factor, or “Rh” factor for short, is present on RBCs. If this factor is present on their red blood cells, that makes the blood type Rh positive; whereas if it’s absent, the blood type is Rh negative. People that are Rh positive can receive both Rh negative or Rh positive blood since they do not have antibodies against the Rh glycoprotein. But if an Rh negative person receives Rh positive blood, they could develop a hemolytic transfusion reaction. Having said that, Rh antibodies require prior exposure to Rh positive RBCs. So, someone who doesn’t have Rh antibodies, won’t have a transfusion reaction the first time they’re exposed to Rh positive blood. However, they develop anti-Rh antibodies, so if they’re exposed to Rh positive blood a second time, that will cause a transfusion reaction.
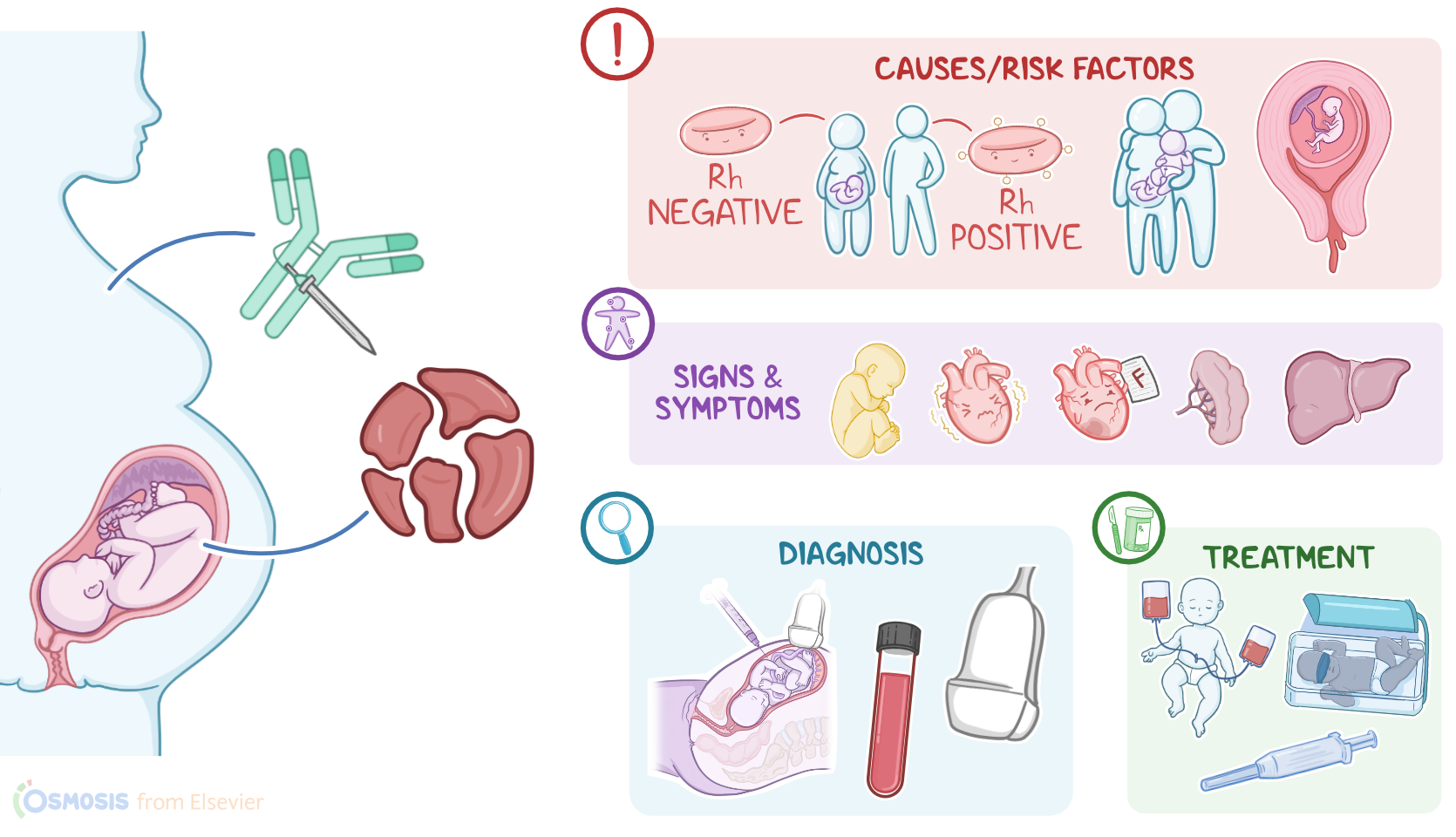
Now, the hemolytic disease of the newborn is mediated by the immune system and can occur when fetal erythrocytes, which express an RBC antigen not expressed on maternal RBCs, breach into maternal circulation, usually when placenta separates at birth. This most commonly occurs due to Rh incompatibility; less commonly, it can be due to ABO incompatibility between the mother and the fetus. Risk factors include the mother being Rh negative while the conceiving partner is Rh positive; second or higher pregnancy; previous pregnancies with hemolytic disease; previous miscarriages or pregnancy complications; Caucasian race; pregnant individuals that have not been tested or received prevention with Rh immunoglobulin; and invasive medical procedures like amniocentesis or chorionic villous sampling.
Pathology-wise, if the baby’s RBCs have any the ABO or Rh glycoproteins that the mother’s immune system hasn’t previously encountered, then these glycoproteins can act as antigens, causing the mother’s immune system to produce antibodies against them. Now, in a first pregnancy, this does not affect the fetus. However, in a subsequent pregnancy, if the fetus is again positive for the same glycoprotein, like, for example, if the fetus is Rh positive, then the mother’s immune system mounts a fast and specific attack against the fetal RBCs, causing hemolysis. Now, hemolytic disease of the fetus and newborn has significant consequences during pregnancy and after delivery. During pregnancy, hemolysis can result in mild fetal anemia, which can cause fetal tachycardia. In case of severe anemia, fetal heart failure can result, causing a buildup of fluids in various organs and tissues, including pericardial effusion, pleural effusion, abdominal ascites, as well as liver and spleen enlargement. This is a condition called hydrops fetalis, and it can be fatal. Moreover, as bilirubin starts to accumulate secondary to hemoglobin breakdown, hyperbilirubinemia develops too, causing jaundice. In utero, jaundice can be seen as a yellow discoloration of the amniotic fluid or umbilical cord. After birth, bilirubin buildup can damage the brain, a condition called kernicterus.
The presentation after birth varies depending on the severity of the hemolysis. With mild anemia, the infant’s vital signs are usually normal, and jaundice develops within 24 hours after birth. Moderate anemia can cause pallor, tachycardia, and jaundice, also within the first 24 hours of life. If the anemia is severe and the baby develops hydrops fetalis, there could be edema or swelling of the entire body, extreme pallor, and significant difficulty in breathing due to heart failure. On palpation, there could also be an enlarged liver and spleen. Diagnosis of hemolytic disease of the fetus and newborn starts with a thorough history and physical examination. During pregnancy, diagnosis can begin with blood typing for ABO and Rh status of the parents early in the first trimester. Fetal blood type and the presence of antibodies against fetal RBCs can also be determined, typically through amniocentesis.
This procedure can also be used to measure bilirubin levels in the amniotic fluid. A prenatal ultrasound can also help identify signs of hydrops fetalis or organ enlargement. After birth, diagnosis of hemolytic disease is confirmed with either a positive direct or indirect antiglobulin test, like the Coombs test, which will confirm the presence of maternal RBC antibodies in the infant’s serum. Additionally, the baby’s blood can be tested for type; a CBC may show low hemoglobin and RBC levels, and high reticulocyte count. A peripheral blood smear often shows evidence of hemolysis, and serum bilirubin levels are usually high. Imaging techniques can also be useful to identify neonatal hydrops fetalis or organ enlargement.