Hepatitis: Nursing
Notes
| HEPATITIS | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
| CAUSES AND RISK FACTORS |
| |
| PATHOPHYSIOLOGY |
| |
| SIGNS AND SYMPTOMS |
| |
| DIAGNOSIS |
| |
| TREATMENT |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
Transcript
Hepatitis refers to an inflammation of the liver due to infection or injury, and it’s often self-limiting, but some cases can result in extensive liver damage.
Now, let’s quickly review some anatomy and physiology. The liver is a large, solid organ located in the right upper quadrant of the abdomen, which has several functions, including the production of bile, cholesterol, and certain blood proteins like albumin and clotting factors; as well as helping with glucose and fat metabolism; detoxification through medication and alcohol metabolism; and it also plays a big role in bilirubin metabolism.
Now, hepatitis can be caused by a viral infection, called viral hepatitis, or other kinds of injury, in which case it’s called non-viral hepatitis.
The more common one is viral hepatitis, which is caused by hepatitis viruses A, B, C, D, or E. Hepatitis A virus is usually transmitted through the fecal-oral route, through contaminated food or water, or through person-to-person contact; and risk factors include living or working in nursing homes, daycare centers, and living in or traveling to countries with poor access to clean water, sanitation, and hygiene; as well as sexual contact with an infected individual.
Next, we have hepatitis B, C, and D viruses, which are primarily transmitted through blood and other body fluids; so the main risk factors include intravenous drug use, blood transfusions, hemodialysis, and working as a healthcare professional; as well as high-risk sexual behavior, such as having multiple partners or not using protection. Hepatitis B can also be transmitted vertically to the baby before or after birth.
Of note, the hepatitis D virus can’t cause an infection in the absence of hepatitis B virus. So the most important risk factor for a hepatitis D infection is a hepatitis B infection.
Lastly, hepatitis E is transmitted through the fecal-oral route, mostly through consuming contaminated food or water.
On the other hand, non-viral hepatitis can be caused by alcohol, medications like acetaminophen, and exposure to certain chemicals like herbicides. Another important cause is autoimmunity, where the client’s immune system attacks the liver, leading to autoimmune hepatitis. Risk factors for autoimmune hepatitis include being assigned female at birth; as well as having other autoimmune diseases, such as thyroiditis or celiac disease; and a family history of autoimmunity.
Now, the pathology of hepatitis can be classified as acute or chronic. With acute hepatitis, the underlying cause leads to quick and severe damage to the liver, which is usually self-limiting, lasting less than 6 months. However, some clients can develop complications like fulminant hepatitis, which is a life-threatening condition characterized by severe liver function impairment.
On the other hand, with chronic hepatitis, there’s progressive damage to the liver that lasts more than 6 months. So, initially, liver function remains intact, but as damage progresses over time, the liver starts to deteriorate. Liver damage can manifest as hepatic cytolysis, where liver cells are destroyed and leak out enzymes like aspartate transaminase, or AST; alanine transaminase, or ALT; and gamma glutamyl transferase, or GGT. Additionally, when the liver is damaged, it can’t process bilirubin anymore, so this compound builds up in the blood and gets deposited in various tissues around the body.
Now, in the long run, liver damage is followed by a regenerative process that eventually causes fibrosis and scarring of the liver, which can progress to cirrhosis. This further impairs liver function, causing ammonia to build up in the blood. Ammonia buildup is quite dangerous because it can cross the blood-brain barrier, and impair central nervous system function, causing hepatic encephalopathy. Finally, cirrhosis also represents a risk for developing hepatocellular carcinoma.
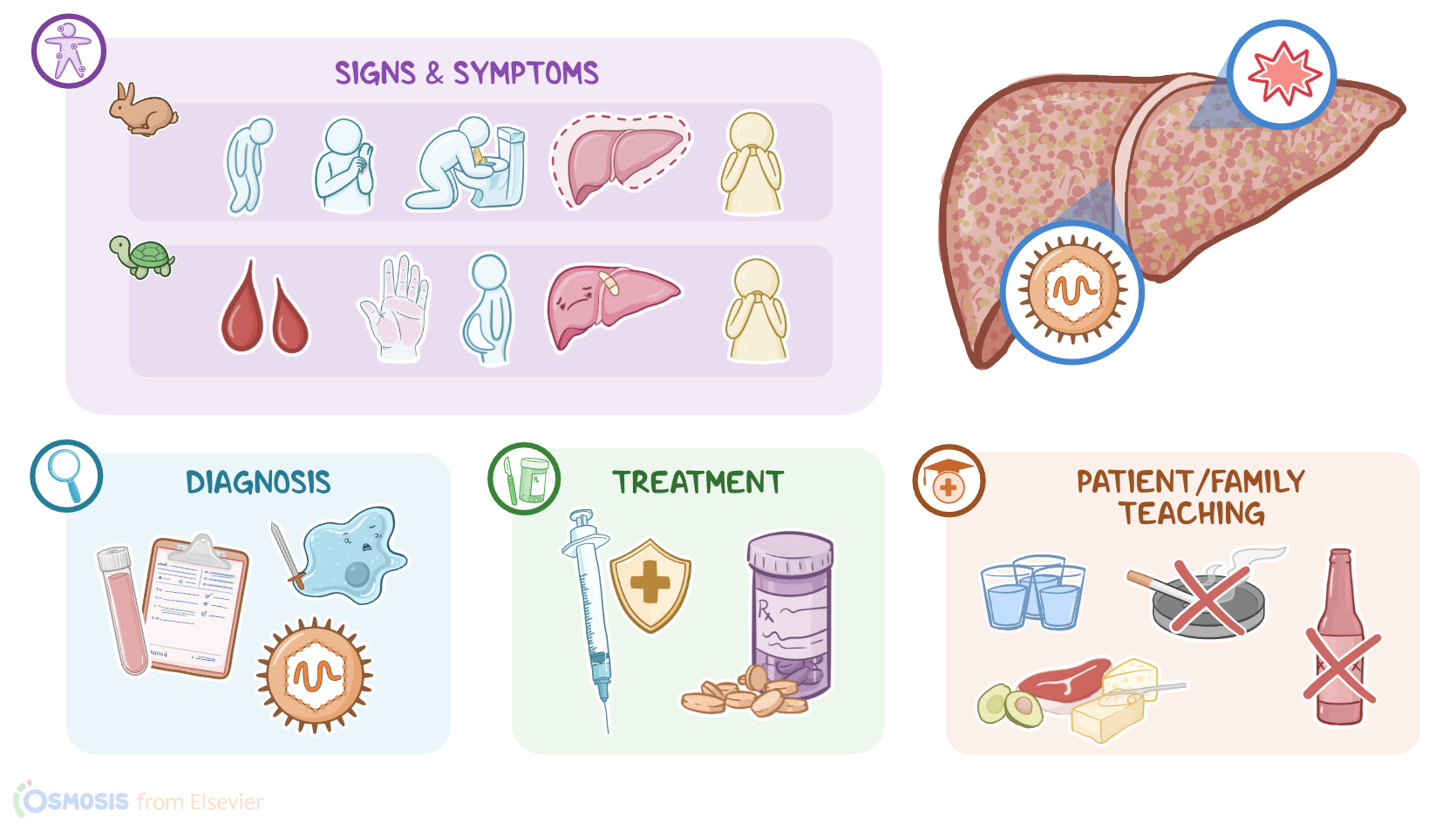
The clinical manifestations associated with acute hepatitis include fatigue, malaise, nausea, and vomiting. Additionally, clients can present with a low-grade fever, jaundice, skin rash, itching, particularly on the palms and soles, as well as dark urine. They may also have right upper quadrant tenderness, as well as hepatomegaly.
On the flip side, clients with chronic hepatitis can initially be asymptomatic, or present with mild symptoms like malaise and fatigue. However, progressive liver damage can, over time, lead to jaundice; as well as ascites, or fluid accumulation in the peritoneal cavity, on account of reduced albumin production; and easy bruising or bleeding because of reduced clotting factors.
On rare occasions, chronic hepatitis can cause gynecomastia or breast enlargement in clients assigned male at birth; as well as skin manifestations, such as palmar erythema and spider angiomas. Sometimes, there can be signs of encephalopathy, like tremor, confusion, somnolence or coma.
Diagnosis of hepatitis starts with the client’s history and physical assessment. Laboratory tests typically reveal elevated liver enzymes like aspartate transaminase, or AST and alanine aminotransferase or ALT; as well as elevated bilirubin levels; and prolonged bleeding time. With chronic hepatitis, sometimes there can be increased ammonia levels in the blood. Additionally, lab tests can also help find the underlying cause of hepatitis. With autoimmune hepatitis, there can be high titers of autoantibodies like ANA and SMA. On the flip side, in case of viral hepatitis, lab tests can reveal specific serologic findings.
First, acute hepatitis A infection is associated with anti-HAV IgM antibodies; while clients with resolved hepatitis A infection or immunization will have anti-HAV IgG antibodies; and HAV doesn’t cause chronic infection. Next up, acute hepatitis B infection presents with hepatitis B surface antigen or HBsAg; as well as IgM antibodies against hepatitis B core antigen. Clients with chronic hepatitis B infection present the same serologic markers, but instead of IgM antibodies, they have IgG antibodies against hepatitis B core antigen. And lastly, clients with resolved hepatitis B infection present with positive IgG antibodies against hepatitis B core antigen and against HBs antigen, but negative HBs antigen. It’s important to note that vaccinated clients only have IgG antibodies against HBs antigen, which composes the vaccine against hepatitis B virus. Moving on, acute and chronic hepatitis C infection can be diagnosed using the HCV antibody test, which detects antibodies to the hepatitis C virus in both acute and chronic forms of infection. In acute and chronic hepatitis D infection, serology reveals either IgM or IgG HDV antibodies, in addition to specific markers of hepatitis B infection. Lastly, acute hepatitis E infection is associated with anti-HEV IgM antibodies; while clients with resolved infection or immunization will have anti-HEV IgG antibodies.