Herpes zoster: Nursing
Herpes zoster: Nursing
test2
test2
Notes
| HERPES ZOSTER | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
| CAUSES AND RISK FACTORS |
| |
| PATHOPHYSIOLOGY |
| |
| SIGNS AND SYMPTOMS |
| |
| DIAGNOSIS |
| |
| TREATMENT |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
Transcript
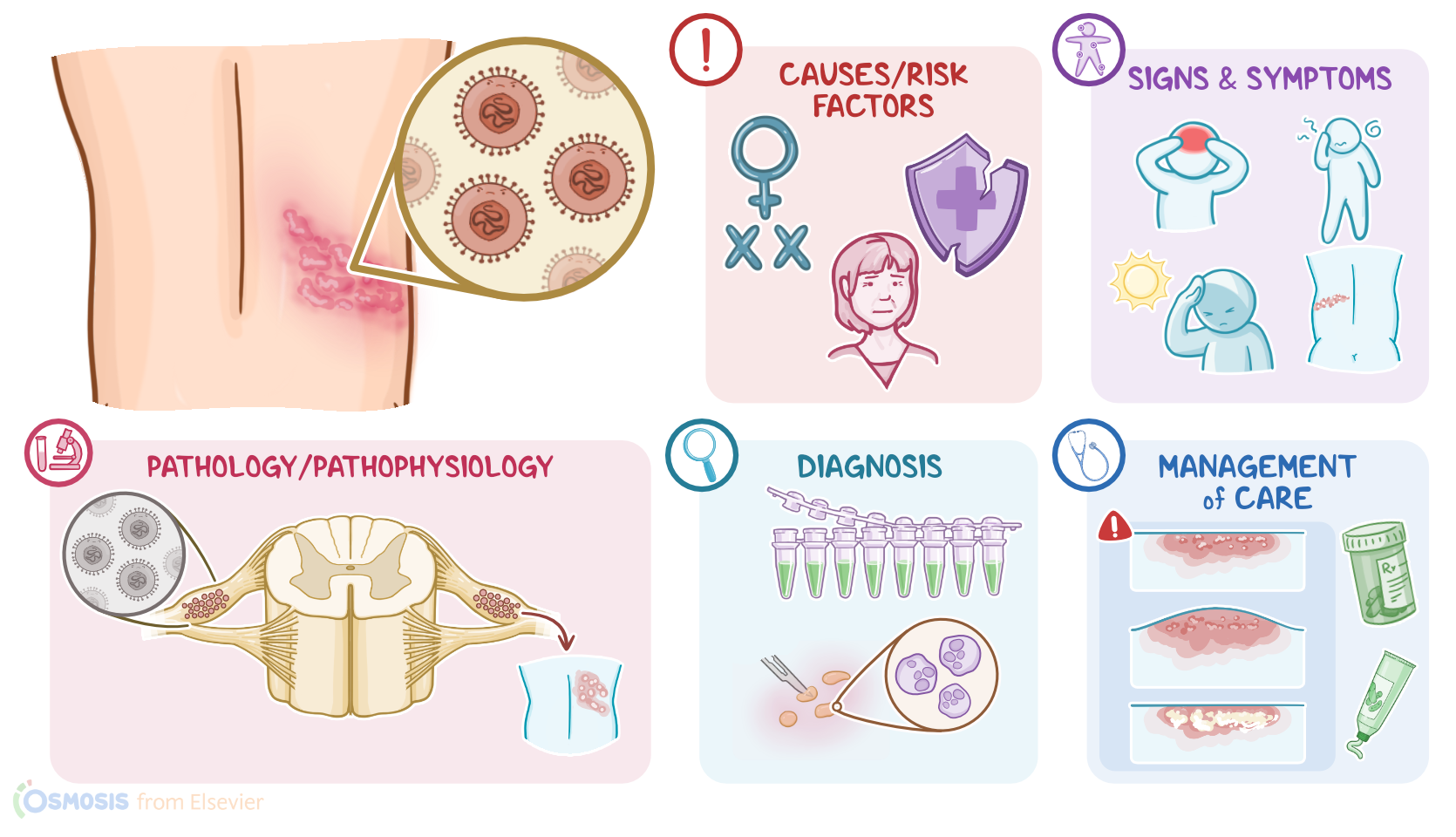
Herpes zoster, also known as shingles, is a painful, blistering rash on a localized area of the skin that is caused by the reactivation of the varicella zoster virus, or VZV. This virus initially causes a disease called varicella, or chickenpox, and can lay dormant in nervous ganglia around the body for many years before reactivation.
Now, let’s quickly recap the physiology of the nervous system, which is divided into the central nervous system, including the brain and spinal cord, and the peripheral nervous system, which includes all the nerves that connect the central nervous system to the skin, muscles, and organs.
Peripheral nerves that originate from the brain are called cranial nerves, and they’re in charge of motor and sensory innervation of the head and neck. A specific cranial nerve, called cranial nerve V, or the trigeminal nerve, is responsible for the sensation in the face. Its sensory neurons create a nerve cell cluster called the trigeminal ganglion, located in the bones on the side of the face between the eyes and ears.
Another cranial nerve, cranial nerve VII, also known as the facial nerve, innervates the muscles of the face.
The peripheral nerves originating from the spinal cord are called the spinal nerves. Each nerve is formed by a dorsal and a ventral root. Ventral roots contain neurons that carry motor innervation from the spinal cord to the muscles. Sensory information, like touch, temperature, pain, and pressure from the skin and other tissues travel through 1st order sensory neurons, in the dorsal root ganglion near the spinal cord, then through the dorsal root, and into the spinal cord, where it synapses with the 2nd order neurons. Now, each spinal nerve is in charge of the sensation of a specific area of the skin, called a dermatome.
Now, herpes zoster is caused by the varicella zoster virus, also known as human herpesvirus 3 or HHV-3 for short, which is a DNA virus that belongs to the family of Herpesviridae. Important risk factors associated with herpes zoster include being assigned female at birth, clients over 50 years of age, and immunocompromised clients.
Moving on to pathology. Varicella zoster virus is a highly contagious airborne virus, meaning it spreads via small virus-containing droplets that get flung in the air when an infected client coughs or sneezes. If another client breathes in these droplets, or they get in contact with infected surfaces and then touch their eyes or mouth, they can become infected.
Once the virus enters the body, it starts replicating in the epithelial cells. Next, the virus gets collected by immune cells and transported to regional lymph nodes where it continues to replicate.
This is called primary infection or chickenpox. In chickenpox, the varicella zoster virus reaches the skin where it spreads directly from one keratinocyte to another one. In some cases, this can result in the formation of giant multinucleated cells called Tzanck cells.
Additionally, the virus infects sensory neurons of the skin and travels to the trigeminal ganglion in the head and dorsal root ganglion in the trunk. Eventually, the immune system eliminates the viral particles from the body, but ones that reach sensory ganglions can remain dormant in the body and enter a latent state. Now, in clients with weakened immune systems, the varicella zoster virus can reactivate and travel down the sensory neuron and infect the skin of a specific dermatome, causing herpes zoster.
The most common complications of herpes zoster are secondary bacterial infection of the affected dermatome; and postherpetic neuralgia, which refers to a pain in the affected dermatome long after the rash disappears. Postherpetic neuralgia occurs due to viral replication in the dorsal root ganglia, which eventually results in inflammation and necrosis of nerve cell bodies.
Next, the varicella zoster virus can affect cranial nerve VII and cause Bell’s palsy, which is a condition associated with weakness or paralysis of the muscles on one side of the face. Additionally, the involvement of cranial nerve VII can result in herpes zoster oticus, which is characterized by severe ear pain and vesicles around and inside the ear.
The virus can also affect the ophthalmic nerve and cause infection of the eye and surrounding skin. This condition is called herpes zoster ophthalmicus and, in severe cases, it can be followed by acute retinal necrosis.
Finally, the varicella zoster virus can spread to the central nervous system and cause meningitis and encephalitis.
Now, clinical manifestations of herpes zoster are often preceded by prodrome symptoms, which can begin days before the herpes zoster itself, and include headache, malaise, and photophobia, as well as a burning pain, or paresthesia in the dermatome that’s affected.
Now, clinical manifestations of the herpes zoster itself typically include a sharply demarcated vesicular rash that looks like a single stripe on one side of the face or the body. It’s important to note that after reactivation of the varicella zoster virus, immunocompromised clients can develop disseminated zoster, which is associated with a vesicular rash that is not limited to a single dermatome but rather affects three or more dermatomes.