Muscular dystrophies - Duchenne and Becker: Nursing
Muscular dystrophies are a group of genetic disorders characterized by progressive muscle degeneration and weakness. There are several types of muscular dystrophies, but the two most common ones are Duchenne and Becker muscular dystrophy. All right, let’s review some anatomy and physiology. The muscular system consists of skeletal or striated muscles, which are attached to bones and contract under voluntary control; as well as smooth muscles found in the walls of hollow organs, and cardiac muscles, which are only found in the heart, and both of which function under involuntary control. Now, a protein, called dystrophin, is normally found on the membrane of muscle cells, primarily skeletal and cardiac, where it provides mechanical support and stabilization.
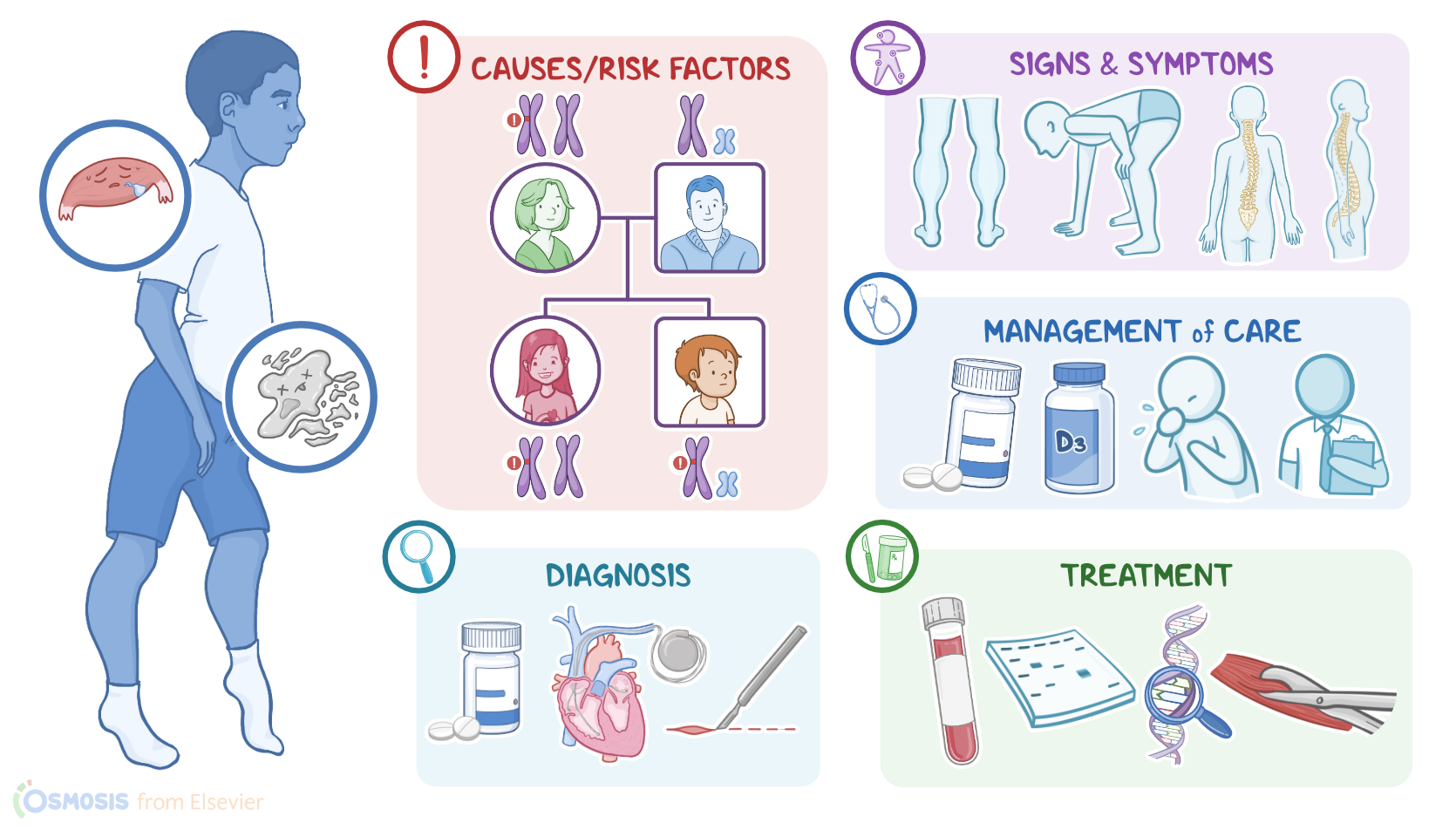
Now, both Duchenne and Becker muscular dystrophies are caused by mutations in the gene that codes for the dystrophin protein. In Duchenne muscular dystrophy, dystrophin is completely absent; whereas in Becker muscular dystrophy, there is some dystrophin present, but it does not function properly. Now, Duchenne and Becker muscle dystrophies are X-linked recessive genetic disorders, so they occur almost exclusively in those assigned male at birth. This is because the dystrophin gene is located in the X-chromosome. So, let’s say a mother has 1 mutated and 1 normal chromosome. She passes down one of the mutated X chromosomes down to her daughter, the father passes down a normal X chromosome, so the daughter is still able to produce functional dystrophin. However, if the mother passes the mutated chromosome to her son and the father passes down a Y chromosome, which doesn’t have the dystrophin gene, the son will not be able to produce functional dystrophin and will develop the disease.
In this case the mother didn’t have the disease, so they're an “asymptomatic carrier. ”Now, pathology-wise, the lack of the dystrophin protein in muscle cells causes them to be fragile and easily damaged. Intracellular proteins like creatine kinase start leaking from the damaged muscle cells, and calcium starts to enter the cell, leading to cell death. In the short term, there is enough muscle regeneration to compensate for the increased muscle degeneration. Unfortunately, over time, the muscle tissue can’t keep up, so it atrophies and gets infiltrated by fat and fibrotic tissue, which results in severe muscle weakness. This process can occur in any muscle, but it is most noticeable in the lower limbs. All right, clinical manifestations of Duchenne muscular dystrophy usually present by age 5. Most children begin to walk later in childhood and have a “waddling” gait with frequent falls. They can also develop calf pseudohypertrophy, meaning their muscles look large, especially in the calves, but it’s actually due to a buildup of fat deposits and fibrotic tissue that accumulates as the muscle cells die.
Another classic sign of Duchenne is the Gowers sign, where a child who’s sitting or lying down can only stand up by first getting on their hands and knees, then slowly bringing their hands towards their feet to stand up. This is due to muscle weakness around the hips and upper legs. Clients can also develop skeletal deformities like scoliosis or hyperlordosis, and growth velocity is usually slower, resulting in a shorter overall stature. Clinical manifestations of Becker muscular dystrophy are similar to those of Duchenne, but are typically less severe and appear later in life, between age 10 to 20. Eventually, clients with Duchenne or Becker muscle dystrophies end up developing serious complications. These include respiratory failure as the diaphragm muscle weakens, as well as dilated cardiomyopathy and arrhythmias, leading to a shortened lifespan. Most clients with Duchenne die in their 20s, and those with Becker in their 40s. The diagnosis of Duchenne and Becker muscular dystrophies starts with the client’s history and physical assessment. Lab tests may show high creatine kinase levels, as well as other muscle enzymes such as aspartate transaminase and alanine transaminase, which indicates increased muscle degeneration. The diagnosis can be confirmed either by a Western blot, which can quantify dystrophin in muscle cells, or genetic tests, which look for mutations in the dystrophin gene.
| MUSCULAR DYSTROPHIES - DUCHENNE AND BECKER | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
| CAUSES AND RISK FACTORS |
| |
| PATHOPHYSIOLOGY |
| |
| SIGNS AND SYMPTOMS |
| |
| DIAGNOSIS |
| |
| TREATMENT |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
No notes for this video yet
Try adding a note below