Neonatal abstinence syndrome: Nursing
Notes
| NEONATAL ABSTINENCE SYNDROME | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
| CAUSES AND RISK FACTORS |
| |
| PATHOPHYSIOLOGY |
| |
| SIGNS AND SYMPTOMS |
| |
| DIAGNOSIS |
| |
| TREATMENT |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
Transcript
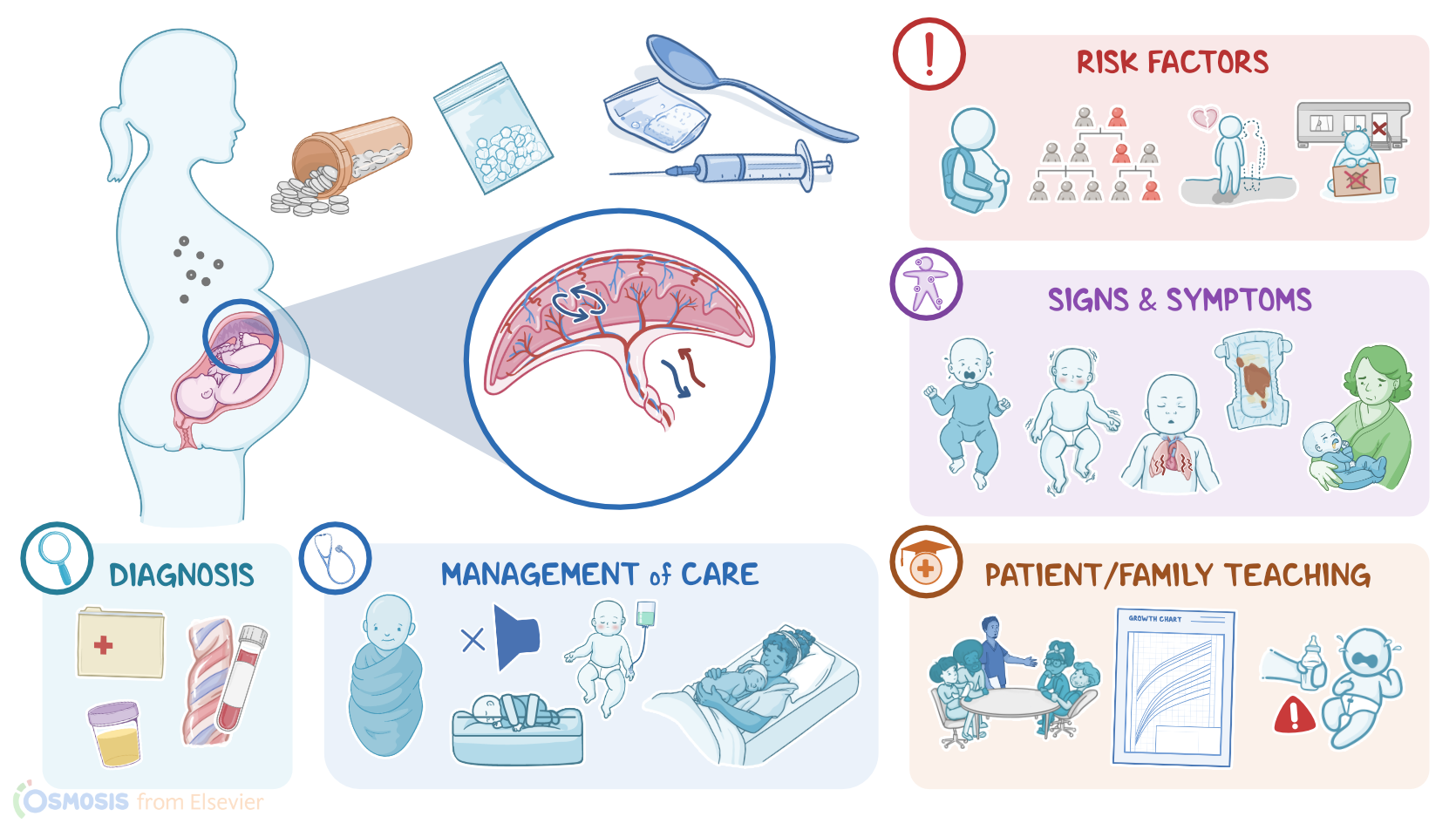
Neonatal abstinence syndrome or NAS for short, is a postnatal withdrawal syndrome that refers to signs and symptoms that a neonate experiences as they withdraw from prenatal exposure to certain substances, most commonly opioids. NAS is characterized by central nervous system hyperirritability, autonomic dysfunction, and gastrointestinal hyperactivity. NAS is also referred to as neonatal opioid withdrawal syndrome, or NOWS for short.
Okay, first, let’s review the physiology of the placenta, which is an organ that’s co-created by the fetus and the mother during development. Zooming in, the placenta can be subdivided into two layers: the maternal layer called the decidua basalis and the fetal layer called the chorion. The decidua basalis looks like a flattened bag of blood with uterine arteries delivering blood in and uterine veins pulling blood out. Then, there’s the chorion, which consists of fingerlike projections called chorionic villi. These villi contain tiny fetal arterioles and venules, and push into decidua basalis, reaching into a warm pool of maternal blood.
Gasses, nutrients, and other substances move back and forth between the decidua basalis and the fetal vessels, by diffusing through the intervillous spaces, which are the spaces between the chorionic villi. So, from there, oxygenated maternal blood, as well as nutrients, and substances can travel through the umbilical vein to the fetal circulation. Eventually, deoxygenated blood will head back towards the placenta through two umbilical arteries. That umbilical vein and the two umbilical arteries collectively form the vessels of the umbilical cord.
The most common cause of NAS is maternal use of opioid substances, such as heroin, morphine, or methadone, and sedative medications, like benzodiazepines, barbiturates, and antidepressants.
Now, the factors that increase the risk of NAS, are also the factors that increase the risk of maternal substance use. Individual risk factors can include young age, poor stress management, and challenges during childhood and adulthood, as well as family history of substance use or mental health conditions. In addition, there are social risk factors, which include a lower educational status, lack of an intimate partner, and unstable relationships or home environment.
Moving on to the pathology of NAS. It starts when a pregnant client uses a substance which enters the maternal circulation, where some amount of this substance reaches the placenta, crosses the intervillous spaces, and eventually enters the fetal circulation. It's important to note that the fetal liver is still immature, thus is unable to metabolize these substances efficiently, which keeps the fetus exposed for prolonged periods. So, with constant exposure to the substance, the fetus becomes dependent on the substance. Upon delivery, the concentration of a specific substance in the infant’s system drops abruptly, leading to substance withdrawal. This can result in central nervous system hyperirritability, autonomic dysfunction, and gastrointestinal hyperactivity.
As far as complications go, NAS can cause challenges with memory and problem-solving, as well as long term cognitive, emotional, or behavioral deficits. In severe cases, NAS might result in neonatal death.
In terms of clinical manifestations of NAS, central nervous system hyperirritability can lead to a high-pitched cry, tremor, seizures, and sleep disturbances, as well as frequent sneezing, gagging, or yawning. Additionally, neonates with autonomic instability can present with tachycardia, tachypnea, changes in body temperature, and excessive sweating. Finally, gastrointestinal hyperactivity symptoms may include vomiting, diarrhea, and poor feeding. In severe cases, these can lead to failure to thrive.
Diagnosis of NAS is primarily based on prenatal maternal history, which reveals the use of a specific substance during pregnancy, as well as the clinical presentation of the newborn. Confirmation methods include detection of the specific substance or its metabolite in the maternal blood or urine, as well as neonatal urine, meconium, or cord blood.
Finally, the management of NAS includes both non-pharmacological and pharmacological methods. Non-pharmacological management includes supportive care, like swaddling, and keeping the infant’s environment quiet and dark to avoid overstimulation. In addition, pharmacological management includes substitution therapy, which refers to the administration of medications like morphine, methadone, or phenobarbital.
Alright, let’s look at the nursing care you’ll provide for an infant with neonatal abstinence syndrome. Your priority nursing goal is to provide supportive care.
Begin by instituting a therapeutic environment and establishing seizure precautions. Place the infant in a quiet, dark environment, and cluster your care to provide uninterrupted quiet time and promote sleep.