Otitis media: Nursing
Introduction0:00–0:15
Otitis media refers to inflammation or infection of the middle ear, and can be classified as acute when it lasts less than three weeks, or chronic when it lasts longer.Let’s start with some anatomy and physiology.
Physiology0:15–0:50
The middle ear is a cavity that lies within the temporal bone, just behind the tympanic membrane. It houses three small bones called ossicles, which transmit sound waves from the tympanic membrane to the inner ear.
The middle ear communicates with mastoid air cells, which are air filled cavities within the mastoid part of the temporal bone.
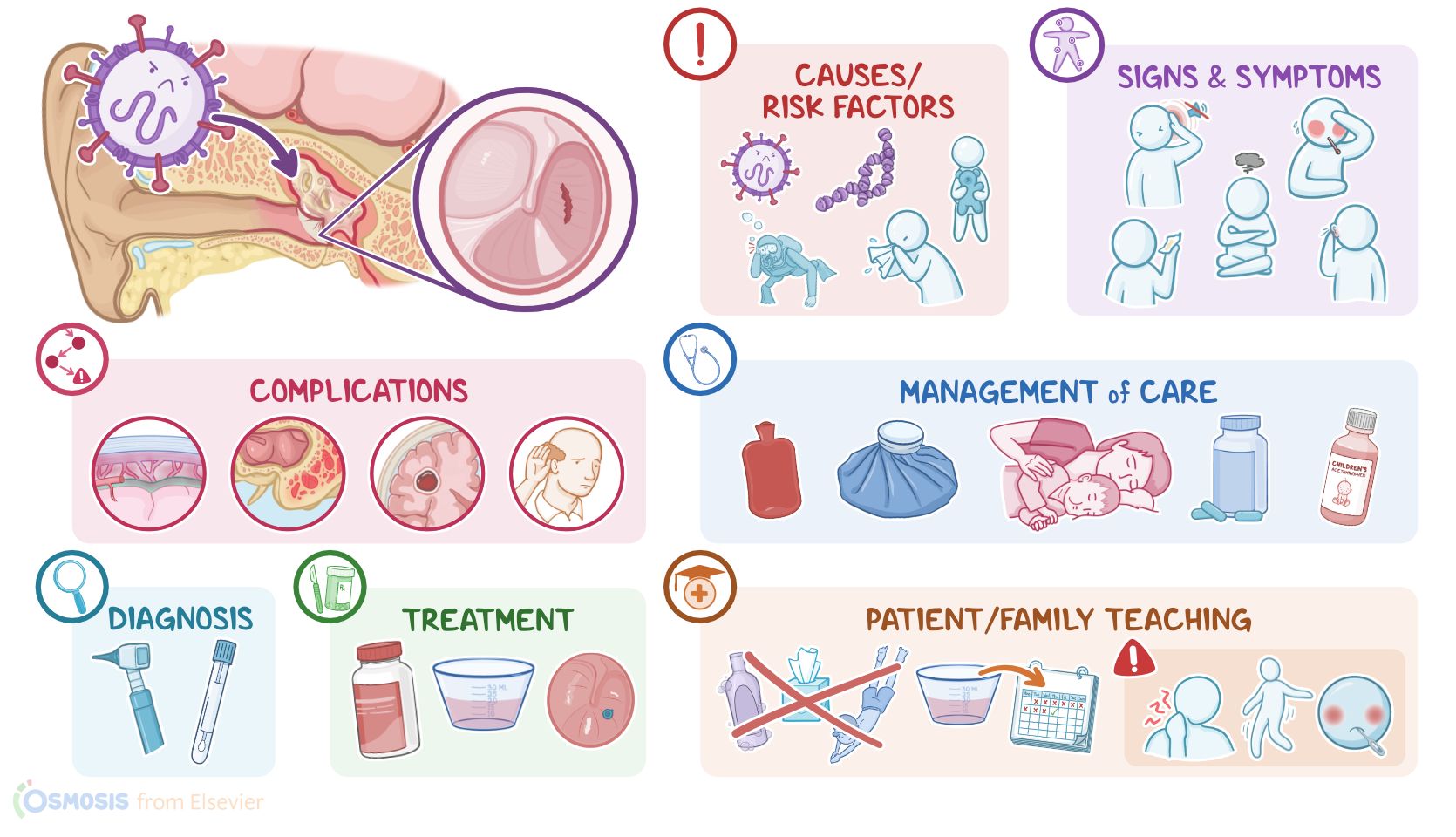
In addition, it communicates with the nasopharynx through the Eustachian tube, which allows air to ventilate the middle ear and normalizes the pressure of the middle ear with the atmospheric pressure.All right, now otitis media is typically caused by viral infections like respiratory syncytial virus, rhinovirus, adenovirus, and coronavirus; or bacterial infections like Streptococcus pneumoniae, Haemophilus influenzae, and Moraxella catarrhalis.
Causes & risk factors0:50–1:55
Risk factors for otitis media include having a cold or upper respiratory infection, chronic sinusitis, and allergies. Other risk factors include dysfunction or anatomic abnormalities of the Eustachian tube, as well as barotrauma, where injury is caused by changes in air or water pressures.
Also, children are at higher risk of otitis media, since their Eustachian tubes are shorter and more horizontal, making it harder for fluid to drain out of the ear and easier for bacteria to climb up into the middle ear.
Lastly, exposure to tobacco smoke increases the risk of otitis media because it impairs the Eustachian tube’s mucociliary function, making respiratory infections more likely.
So the pathology of otitis media occurs when the infection triggers an inflammatory process that obstructs the Eustachian tube.
Pathology1:55–2:42
This results in impaired ventilation of the middle ear, which in turn traps secretions and favors bacterial growth. In addition, the pressure inside the middle ear rises, which may cause the tympanic membrane to bulge or even perforate.
Now, complications of otitis media include hearing loss, as well as complications that occur when the infection spreads to nearby areas.
These include mastoiditis when the infection extends to the mastoid bone and mastoid air cells; meningitis when it extends to the meninges; or even a brain abscess if it extends to the brain or cerebellum.
Clinical manifestations2:42–3:01
The typical clinical manifestations of otitis media include ear pain and fever. In addition, clients with tympanic membrane perforation may present with discharge or drainage, as well as impaired hearing.
In infants and young children, additional symptoms may include irritability and repeated tugging of the ear.The diagnosis of otitis media starts with the client’s history and physical assessment.
Diagnosis3:01–3:29
This includes otoscopic examination of the tympanic membrane, which may appear red, bulging, retracted, or even perforated.
If there’s discharge or drainage from the ear, a culture can be done to determine the causative microbe. Finally, in certain cases, imaging like CT scan or MRI of the head can be performed to assess spreading of the infection.Now, treatment-wise, mild cases of acute otitis media can be managed conservatively, with watchful waiting.
Treatment3:29–4:40
This means only administering symptomatic medications, usually ibuprofen and acetaminophen, to address the fever and pain.
It is indicated in children older than 24 months, that are otherwise healthy and only have mild pain and fever. More severe cases of acute otitis media can require oral antibiotics for the infection.
On the other hand, treatment of chronic otitis media typically includes topical and oral antibiotics. Clients with persistent infection despite antibiotics may require myringotomy, or surgical incision of the tympanic membrane to relieve pressure; as well as tympanostomy, where a tube is inserted through the tympanic membrane to ventilate the middle ear and drain fluid.
Clients with tympanic membrane perforation can be treated with tympanoplasty, where the perforation is surgically repaired.
Lastly, if the client develops mastoiditis, a mastoidectomy can be performed to surgically remove the mastoid air cells.All right, let’s look at the nursing care you’ll be providing for a child with otitis media.
Management and care4:40–5:25
Priority goals of care include pain management and preventing complications. Begin by assessing their temperature and level of pain using a pain scale like the FLACC scale.
Administer the prescribed antipyretic, analgesic and antibiotic medications, and implement comfort measures by providing warm heat or a cool compress and have the child lay on their side with the affected ear down.
If the child experiences a sudden onset of severe pain, followed by immediate relief, as well as the presence of drainage from the ear canal, report these findings to the healthcare provider as this may indicate a perforated eardrum.
Okay, let’s move on to client and family teaching. First, review your client’s plan of care, and provide information about otitis media and their prescribed medications.
General client and family teaching5:25–7:10
Teach them to give their child the prescribed analgesic exactly as directed, and that a warm, moist face cloth placed on the ear may help relieve pain as well.
Be sure to stress to the child’s caregivers the importance of completing the entire dose of antibiotics, even if the child starts to feel better.
If your client has tympanostomy tubes placed, teach the caregiver that the tubes usually fall out on their own after several months; however they should let the healthcare provider know if the tubes fall out.
Lastly, be sure to explain that they should avoid blowing their nose for 7 to 10 days after surgery since this can increase ear pressure, forcing infectious organisms up the Eustachian tube.
Next, review how to prevent future ear infections. Encourage breastfeeding for at least the first 6 months of life, and if bottle feeding, always feed the infant in an upright position.
Also let them know to avoid exposure to tobacco smoke and known allergens, and stay up to date on all vaccinations. Lastly, be sure to emphasize the importance of contacting the provider if the child’s symptoms do not improve within 48 hours; or if they develop new symptoms such as increased discharge from the ear; increased fever; headache; neck pain; hearing loss; swelling around the ear; impaired balance or motor problems; or weakness of facial muscles.All right, as a quick recap ….
Review7:10–8:45
Otitis media is inflammation of the middle ear, which is typically caused by viral infections like respiratory syncytial virus, rhinovirus, adenovirus, and coronavirus; or bacterial infections like Streptococcus pneumoniae, Haemophilus influenzae, and Moraxella catarrhalis.
Children are at increased risk of developing otitis media because they have shorter and more horizontal Eustachian tubes, which makes it harder for liquid to drain out of the ear, and easier for microbes to find their way into the middle ear.
Diagnosis involves history and physical assessment as well as otoscopic examination of the tympanic membrane. Treatment for mild acute infections can rely on watchful waiting, which only involves symptomatic medication like ibuprofen or acetaminophen.
More severe cases of acute otitis media can benefit from oral antibiotics, while treatment for chronic otitis media usually relies on both topical and oral antibiotics.
Other treatment measures include myringotomy, tympanoplasty, mastoidectomy, and tympanostomy where a tube is inserted through the tympanic membrane to ventilate the middle ear and drain fluid.
The priority goals of care include pain management and preventing complications. Client and family teaching focuses on understanding the prescribed treatment plan, prevention of recurrence, and knowing when to contact the healthcare provider.
| OTITIS MEDIA | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
| CAUSES AND RISK FACTORS |
| |
| PATHOPHYSIOLOGY |
| |
| SIGNS AND SYMPTOMS |
| |
| DIAGNOSIS |
| |
| TREATMENT |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
- "Medical-surgical nursing: Concepts for interprofessional collaborative care" Elsevier (2021)
- "Lewis’s medical-surgical nursing: Assessment and management of clinical problems" Elsevier (2020)
- "Saunders comprehensive review for the NCLEX-RN examination" Elsevier (2018)
- "Evidence Assessment of Management of Acute Otitis Media: I. The Role of Antibiotics in Treatment of Uncomplicated Acute Otitis Media" Pediatrics (2001)
- "Clinical practice guidelines for the diagnosis and management of acute otitis media in children—2018 update" Auris Nasus Larynx (2020)
- "Antibiotic Recommendations for Acute Otitis Media and Acute Bacterial Sinusitis" Pediatric Infectious Disease Journal (2018)
No notes for this video yet
Try adding a note below