Pediculosis and scabies: Nursing
Notes
| PEDICULOSIS AND SCABIES | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
| CAUSES AND RISK FACTORS |
| |
| PATHOPHYSIOLOGY |
| |
| SIGNS AND SYMPTOMS |
| |
| DIAGNOSIS |
| |
| TREATMENT |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
Transcript
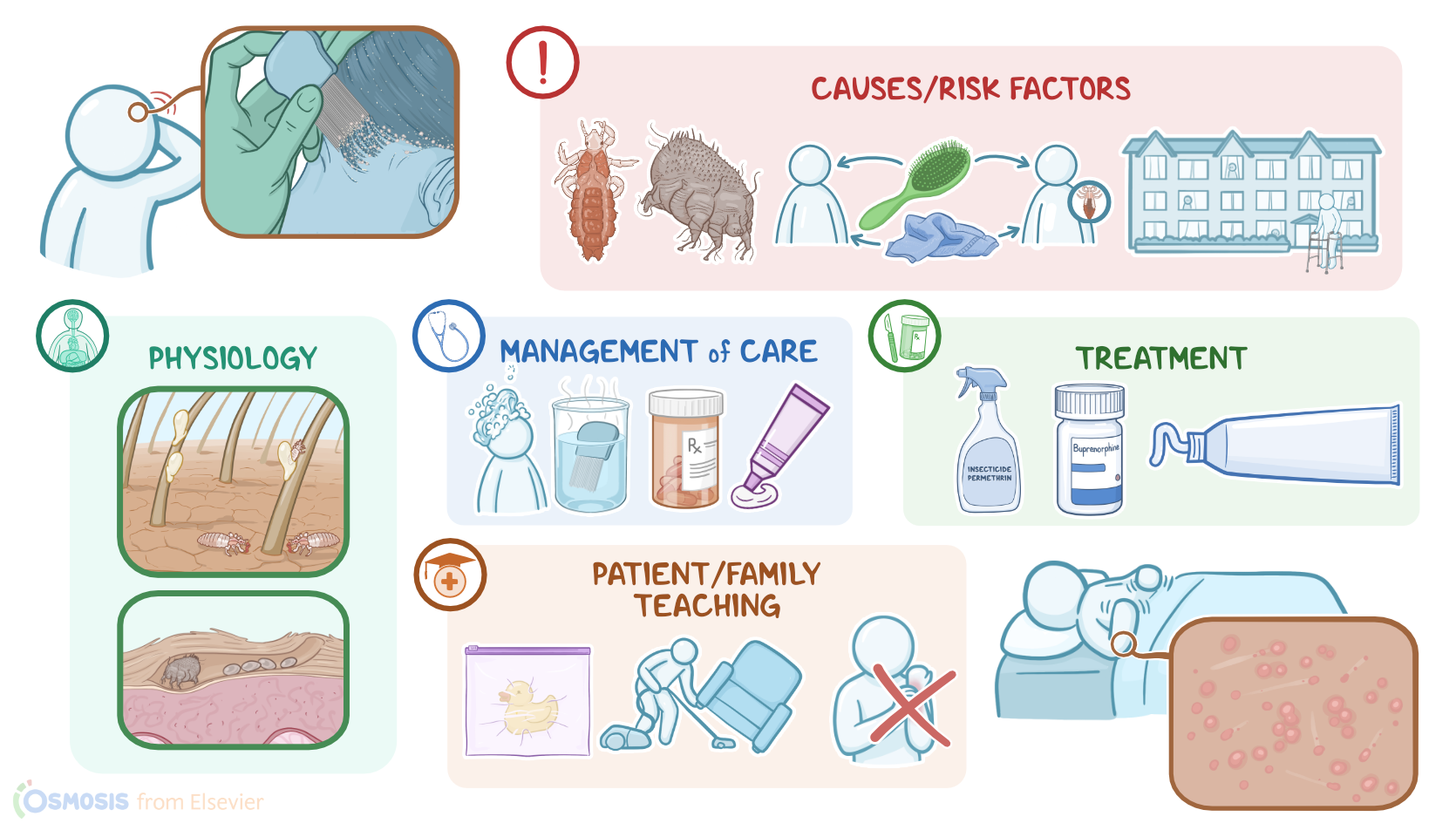
Pediculosis and scabies are both parasitic skin disorders. Pediculosis is an itchy infestation of the lice in hairy parts of the head or body, while scabies is a skin infection caused by an infestation of mites called Sarcoptes scabiei.
Let’s start by looking at the anatomy and physiology of the skin. The skin is made of the epidermis, which is an outer layer that acts as a protective barrier against the environment; the dermis, which primarily contains blood vessels and nerve endings; and the hypodermis, which is a layer of connective tissue that provides structural support to the skin. Hair follicles begin in the dermis, and hair grows out of these follicles in most body areas. The visible part of the hair is called the hair shaft.
Now, pediculosis is caused by different lice species: head lice called Pediculus humanus capitis; body lice, or Pediculus humanus; and pubic or crab lice, called Phthirus pubis. Meanwhile, scabies is always caused by Sarcoptes scabiei.
One of the largest risk factors for contracting pediculosis or scabies is having close contact with an affected individual. This commonly happens among children in school, especially head lice. Other risk factors for pediculosis include sharing personal items, like brushes or towels, as well as having sexual intercourse with an affected individual. Risk factors for scabies include living in an institutionalized setting, like prison or a long-term care facility, or being a refugee or unhoused.
Now let’s switch gears and look at the pathology of pediculosis. This condition starts after direct contact with a person who is infected with lice, or indirect contact through sharing personal items. Next, the female lice lays eggs in the hair shaft, and then the growing and adult lice suck blood from the individual’s skin. Saliva and fecal matter from the lice leads to inflammation and itching.
Scabies is almost always transmitted by direct physical contact. The female mites burrow into the outer layer of skin forming curved ridges in which they lay their eggs. Clients may have an allergic reaction to the mites, their eggs, and their feces, which causes the red, bumpy and extremely itchy papules.
Typically, the clinical manifestations of both pediculosis and scabies includes intense itching. With pediculosis, itching commonly occurs only in the affected area like the head, and the client may develop excoriation from scratching. Upon assessment, you may find nits that look like small white eggs or lice that look like small gray or tan crawling specks.
In contrast, scabies often causes itching all over the body, except for the face, and it’s typically worse at night. On assessment, there are papules on the skin with curved or linear ridges, along with fine, grayish lines.
Diagnosis of pediculosis and scabies starts with the client’s history and physical assessment. For pediculosis, visualizing the nits or lice is sufficient. However, scabies can be confirmed with a microscopic examination of a scraping from the lesion.
Treatment of pediculosis and scabies begins with topical insecticide medications like permethrin. For pediculosis, a client may instead be given topical benzene hexachloride or spinosad. For scabies, lindane can also be used instead. If the infestation is resistant to the initial topical treatment, then the second line medication for both diseases is oral ivermectin.
Okay, when caring for a client with pediculosis or scabies, your priority goals of nursing care are to prevent the spread of the infestation and promote comfort.