Peptic ulcer disease (PUD): Nursing process (ADPIE)
2,725views
Peptic ulcer disease (PUD): Nursing process (ADPIE)
MS LEC PRELIMS 2nd SEM
MS LEC PRELIMS 2nd SEM
Notes
| PEPTIC ULCER DISEASE (PUD) | ||
| KEY POINTS | NOTES | |
| PATIENT REPORT |
| |
| PATHOPHYSIOLOGY |
| |
| DIAGNOSIS AND TREATMENT |
| |
| ASSESSMENT |
| |
| NURSING DIAGNOSES |
| |
| PLANNING |
| |
| IMPLEMENTATION |
| |
| EVALUATION |
| |
Transcript
Paola Salazar is a 56-year-old hispanic female client admitted to your unit after an esophagogastroduodenoscopy, or EGD, revealed a bleeding gastric ulcer which was controlled by thermal coagulation.
Her recent history includes intermittent upper abdominal pain, and a recent weight loss of five pounds because of nausea and decreased appetite.
After experiencing an episode of hematemesis, her primary care physician, or PCP, ordered an EGD.
A biopsy taken during the procedure is negative for Helicobacter pylori, or H. pylori for short.
Her other health problems include fatigue and chronic back pain.
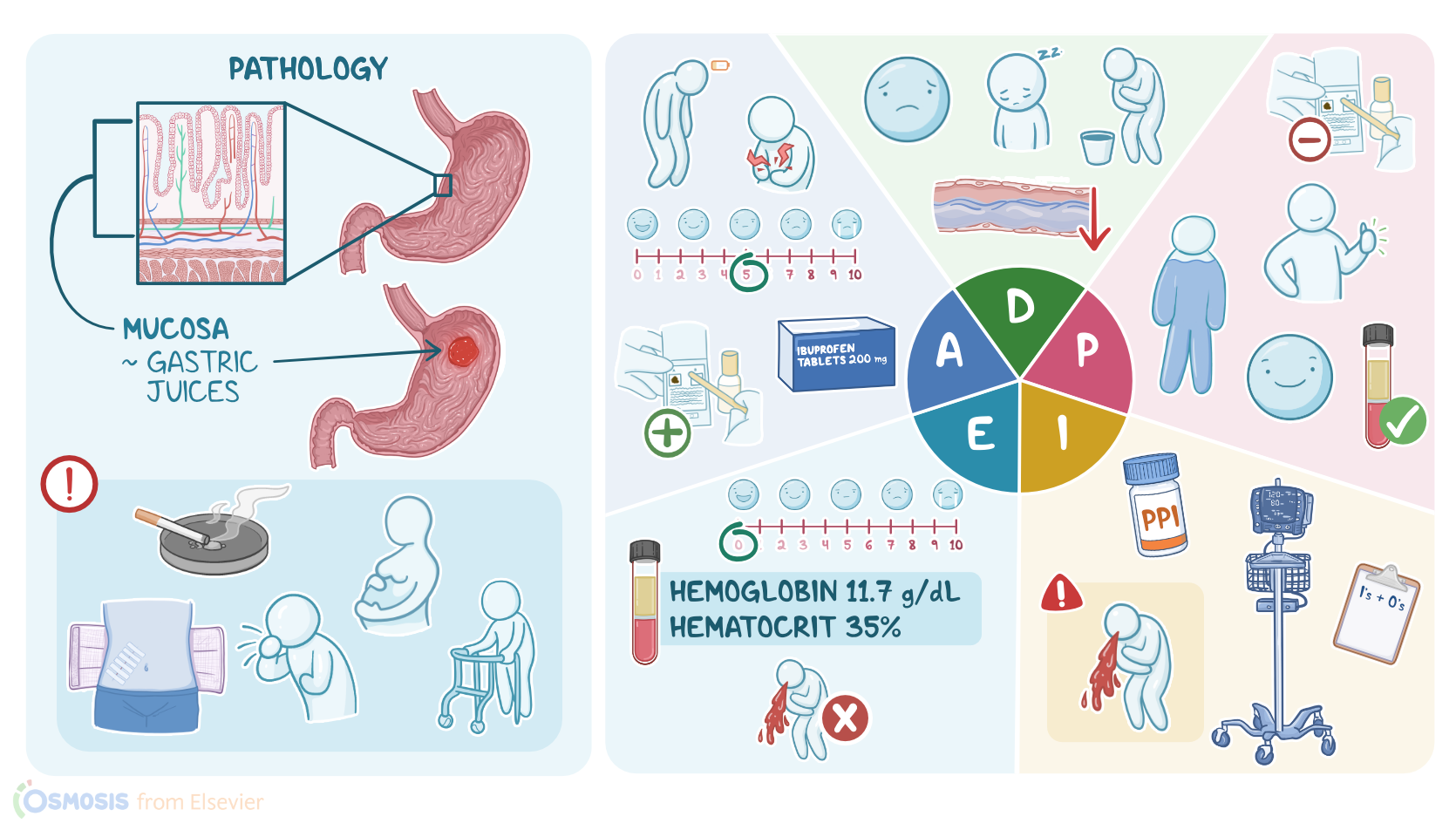
Peptic ulcer disease, or PUD, is an erosion of the lining of the gastrointestinal, or GI tract, most commonly in the proximal duodenum and stomach.
The lining of the GI tract is made of four layers, the mucosa, which is the innermost layer, followed by the submucosa, muscularis, and serosa.
Cells in the mucosa secrete harsh gastric juices, like hydrochloric acid and pepsin, which help digest food.
Normally the mucosa is protected from self-digestion due to tightly joined epithelial cells that resist penetration, and by prostaglandins that stimulate secretion of a protective layer of mucus and bicarbonate.
When the gastric juices overcome these protective mechanisms and damage the gastric lining, a peptic ulcer develops.
Sometimes PUD is asymptomatic, but often the exposure to irritating gastric juices can cause burning epigastric pain.
Typically, pain from gastric ulcers increases 15-30 minutes after a meal, while pain from duodenal ulcers increases 2-3 hours after a meal and at night.
Other common symptoms include bloating, abdominal fullness, and nausea.
If the erosion extends down to the muscularis level it can damage blood vessels resulting in an upper GI bleed, hematemesis, or melena, when blood passes through the lower GI tract, producing a dark, tarry stool.
Anemia from extensive blood loss causes symptoms like fatigue, pallor, and shortness of breath.
Sometimes, an ulcer can perforate through all four layers of the gastric lining and create an opening into the peritoneal cavity.
Free air and gastric contents that enter the abdomen cause peritonitis and findings like severe abdominal pain, abdominal rigidity, and tachycardia.
It is important to keep an eye out for these findings because a perforation requires emergent surgical management.
A major risk factor for developing PUD is infection with H. pylori, which causes an inflammatory response that disrupts protective mechanisms in the gastric mucosa.
Another common cause of PUD is NSAID use because these drugs work by inhibiting prostaglandin synthesis, which is essential for gastric protection.
Reducing the level of prostaglandins over a prolonged period of time leaves the gastric mucosa susceptible to damage, and overtime ulcers can begin to develop.
There are also certain lifestyle choices that can contribute to PUD.
Smoking reduces blood flow to the gastric mucosa and is associated with cell death and poor healing, while alcohol consumption increases cell permeability and weakens the protective mucus barrier.
Other risk factors are African American or Hispanic ethnicity, and having a first degree relative with PUD.
Finally, a rare cause of PUD is Zollinger-Ellison syndrome, which is a gastrin secreting tumor that increases gastric acid production.
Diagnosis of PUD is based on history, physical examination and by EGD which visualizes the lining in the stomach and duodenum.
During the procedure, a biopsy is obtained and analyzed for the presence of H. pylori. H. pylori may also be detected by a urea breath test.
Finally, labs like a CBC or testing for fecal occult blood are used to identify common complications of PUD like bleeding or anemia.
Treatment of PUD depends on the underlying cause and severity of the disease. NSAIDs, if used, are discontinued.
Medications like proton pump inhibitors, or PPIs, and H2-receptor antagonists, or H2RAs, are used to decrease production of stomach acid.
If H. pylori is detected, a triple or quadruple regimen is prescribed that may include a combination of a PPI, certain antibiotics, and bismuth subsalicylate.
For some clients, a prostaglandin analog, like misoprostol is prescribed, while sucralfate is administered in some cases because it forms a protective coating over the ulcer to protect it while it heals.
OK, it is time to start your assessment of Mrs. Salazar, who has just returned from the EGD where hemostasis of her bleeding ulcer was achieved.
Sources
- "Ackley and Ladwig’s Nursing Diagnosis Handbook: An Evidence-Based Guide to Planning Care, 13th edition" Mosby (2022)
- "Harrison’s Principles of Internal Medicine, 21st edition" McGraw Hill / Medical (2022)
- "Evidence-based clinical practice guidelines for peptic ulcer disease 2020" J Gastroenterol (2021)
- "Clinical Guidelines for Drug-Related Peptic Ulcer, 2020 Revised Edition" Gut Liver (2020)
- "Perforated and bleeding peptic ulcer: WSES guidelines" World J Emerg Surg (2020)
- "Health Assessment for Nursing Practice, 7th edition" Elsevier (2021)
- "Upper Gastrointestinal Bleeding in Adults: Evaluation and Management" Am Fam Physician (2021)