Pericarditis: Nursing
Pericarditis: Nursing
Medical Surgical
Medical Surgical
Notes
| PERICARDITIS | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
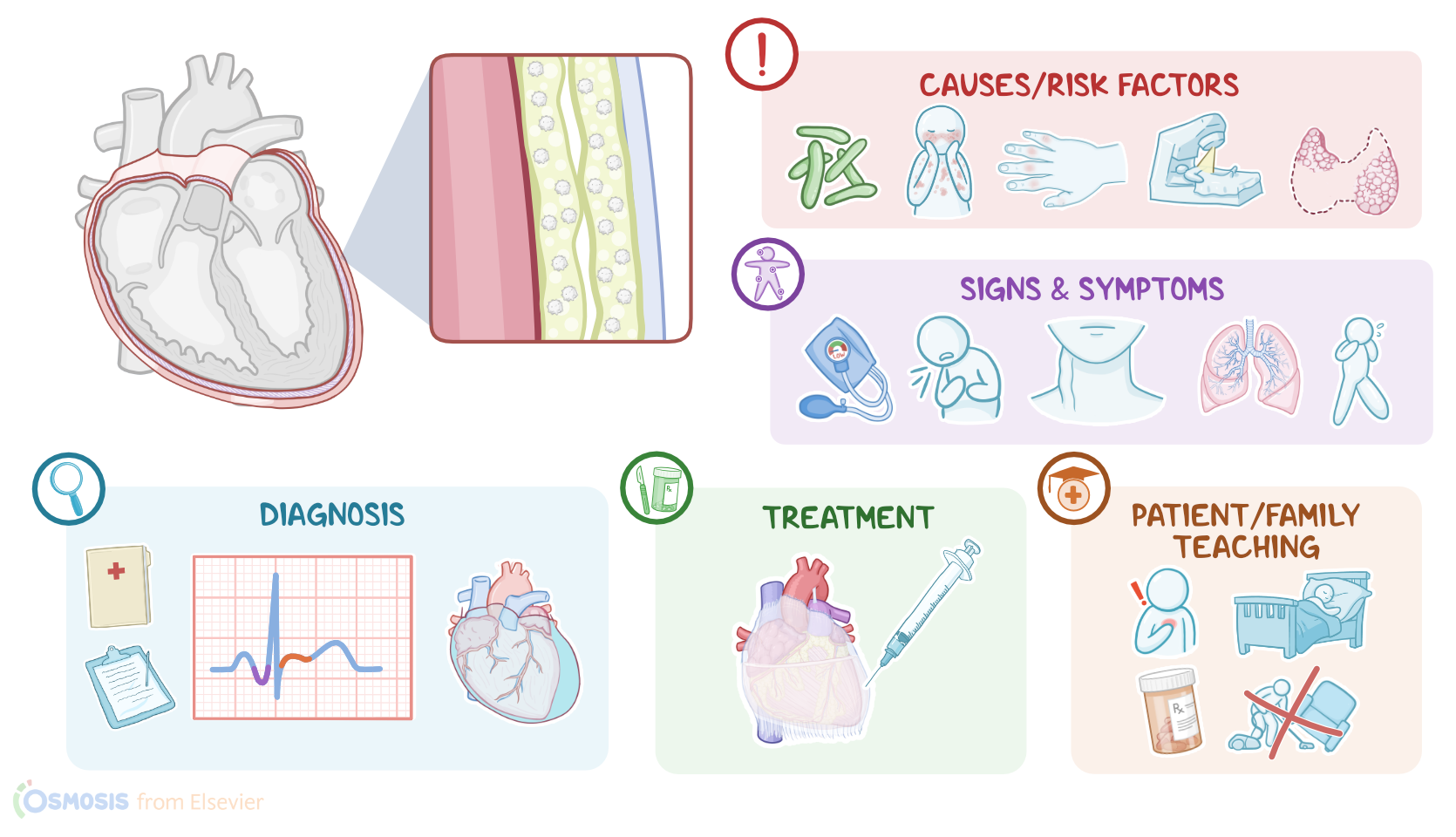
| CAUSES AND RISK FACTORS |
| |
| PATHOPHYSIOLOGY |
| |
| SIGNS AND SYMPTOMS |
| |
| DIAGNOSIS |
| |
| TREATMENT |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
Transcript
Pericarditis refers to inflammation of the pericardium, which is a thin, fibro-elastic sac that surrounds the heart and the roots of the great vessels, cushioning them, and preventing friction during each heartbeat.
Let’s start with a bit of physiology. The pericardium has two layers: an outer fibrous layer, known as the parietal pericardium; and an inner serous layer, called the visceral pericardium. The visceral pericardium is continuous with the parietal pericardium, so they form an enclosed space called the pericardial cavity. Within it, there’s serous pericardial fluid, that is secreted by visceral pericardium cells and drained by parietal pericardial cells and lymphatics, in order to maintain a normal volume of about 5 to 20 mL. The pericardial fluid cushions the heart from any kind of external jerk or shock, and also acts as a lubricant to reduce friction with each heartbeat. The pericardium also fixes the heart to the mediastinum, preventing it from twisting, so that blood circulation through the great vessels doesn’t get cut off.
Now, pericarditis is caused by inflammation of the pericardium, and most cases are idiopathic, meaning that there’s no identifiable cause. When the cause is identified, it’s usually an infection, most commonly a virus, such as Coxsackie B virus or echovirus. Less frequently, pericarditis can be caused by bacteria like Streptococcus pneumoniae or Staphylococcus aureus; as well as fungi like Histoplasma capsulatum and Candida spp.
On the other hand, non-infectious causes of pericarditis include Dressler syndrome, also known as postmyocardial infarction syndrome, which is an immune response triggered by antigens released by dying heart cells, and occurs several weeks after myocardial infarction. Another non-infectious cause of pericarditis is uremia, which is when blood levels of urea get really high, usually due to kidney failure. The high levels of urea irritate the visceral pericardium cells, leading them to secrete a thick pericardial fluid that’s full of fibrin strands and white blood cells.
Pericarditis can also be caused by autoimmune diseases, such as systemic lupus erythematosus, rheumatoid arthritis, or scleroderma. Finally, other causes of pericarditis include cancer and radiation therapy to the chest, as well as severe hypothyroidism and certain medications like penicillin, procainamide, and hydralazine.
Now, pathology-wise, with pericarditis, the pericardial layers are infiltrated by immune cells and fluid. As a result, these layers become inflamed, thicker and boggier - think about how a piece of dry flat pasta gets cooked and thickens up as it soaks up fluid. This makes the layers rub against each other instead of gliding past with each heartbeat. This process can be acute, which develops suddenly and lasts days to weeks; subacute, which lasts weeks to months; or chronic, which usually develops over time and lasts longer than 3 months.
In clients with acute pericarditis, inflammation causes the pericardial blood vessels to be “leakier” than usual, meaning fluid can make its way out of the vessels and into the pericardial cavity, causing a pericardial effusion. This fluid can be serous, meaning the fluid is clear; hemorrhagic, when there’s blood in it; or purulent, if there’s pus in it; and this depends on the cause of pericarditis. Additionally, if the pericardial effusion grows or worsens quickly, it can put pressure on the heart itself, preventing it from fully stretching out or relaxing between contractions. This can cause cardiac tamponade, where the heart can’t fill or pump blood properly, which is a medical emergency.
On the other hand, in clients with chronic pericarditis, the visceral pericardium gradually becomes more and more fibrous, forming a stiff shell that constricts the heart. As a result, it becomes harder for the heart to relax and expand to fill with blood, causing a decrease in cardiac output, which is the amount of blood the heart pumps out with each heartbeat. This is also known as constrictive pericarditis.
Over time, this can lead to heart failure, where the heart is unable to pump enough blood to meet the body’s requirements. Moreover, since blood isn’t being pumped forward, it starts backing up into the pulmonary and systemic circulations. Eventually, this increases the pulmonary blood pressure, and fluid can get into the lung vessels; and also increases the amount of blood in the venous circulation. This causes complications like pulmonary hypertension and peripheral edema, respectively.
Now, the main clinical manifestation of acute pericarditis is severe, sharp retrosternal chest pain, called pericardial pain, which worsens when lying down or taking a deep breath, and improves when the client sits upright and leans forward. This pain can radiate to the neck, shoulders, and back. Upon auscultation, there’s a pericardial friction rub, which is a scratchy, grating, high-pitched rub caused by the heart rubbing against the surrounding pericardium when beating. Sometimes this sound is described as being similar to the sound of sandpaper rubbed on wood. Finally, if the underlying cause is an infection, manifestations can include a fever and chills, amongst others.
Additionally, complications come with their own signs and symptoms. For example, with heart failure, there could be hypotension, on account of decreased cardiac output; and with cardiac tamponade, clinical findings could include pulsus paradoxus. This is when blood pressure drops more than 10 mmHg when the patient breathes in.
On the other hand, chronic pericarditis typically presents with clinical manifestations of right heart failure, including dyspnea, fatigue, and jugular venous distention, where the jugular vein in the neck becomes enlarged and distended. Some clients can develop pulmonary edema, which typically presents with dyspnea and crackles; as well as peripheral edema, causing the limbs to swell.
Diagnosis of pericarditis starts with the client’s history and physical assessment, followed by an ECG, which typically shows initial widespread ST segment elevation, meaning the ST segment is elevated in almost all leads, along with PR segment depression. An important element is to distinguish these findings from an ST elevation myocardial infarction, or STEMI, in which case the ST elevation is typically localized in two or three leads. Additional diagnostic tests include laboratory tests, which can reveal an elevated white blood cell count, as well as an increased ESR and CRP.