Placental abruption: Nursing process (ADPIE)
Placental abruption: Nursing process (ADPIE)
Nursing
Nursing
Notes
| PLACENTAL ABRUPTION | ||
| KEY POINTS | NOTES | |
| PATIENT REPORT |
| |
| PATHOPHYSIOLOGY |
| |
| DIAGNOSIS AND TREATMENT |
| |
| ASSESSMENT |
| |
| NURSING DIAGNOSES |
| |
| PLANNING |
| |
| IMPLEMENTATION |
| |
| EVALUATION |
| |
Transcript
Maria Beam, G2 T0 P0 A1 L0 at 36 weeks of gestation, is a 38-year-old female client who presents to the emergency department with pain in her lower back and uterus.
Maria has a history of smoking and hypertension and she has had no prenatal care for this pregnancy.
Uterine palpation reveals a distended, tender and rigid uterus. Scant vaginal bleeding is present.
Maria is sent to the labor and delivery unit for further assessment and observation.
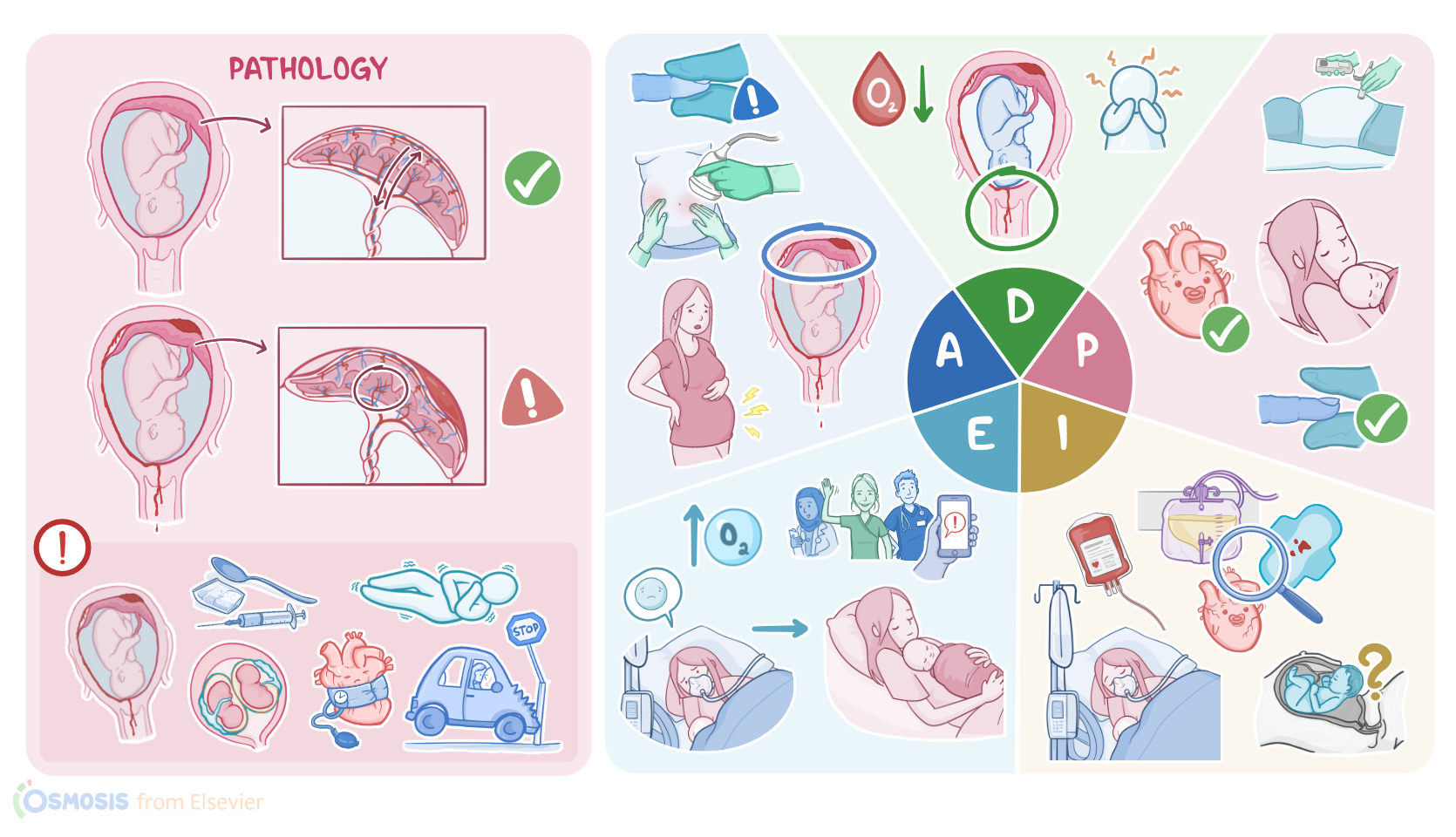
Placental abruption, also referred to as abruptio placentae is a medical emergency where there’s premature detachment of all or part of a normally implanted placenta from the uterine wall, resulting in hemorrhage.
Placental abruption can be classified as complete or partial, depending on the degree of detachment from the uterine wall; as well as apparent or concealed, depending on whether the hemorrhage is seen or not.
This usually happens after about 20 weeks of gestation and affects about 1% of pregnancies worldwide.
Now, the placenta is a temporary organ that forms where the embryo attaches to the uterine wall, and its job is to permit gas and nutrient exchange between the mother and the fetus.
Detachment is usually caused by degeneration of the uterine arteries that supply blood to the placenta, often due to a chronic disease process in the placenta.
The most important risk factors for this include chronic problems like hypertension or smoking.
Also use of certain illicit drugs, like cocaine and methamphetamine can increase the risk of abruption.
Other risk factors include multiple gestation, maternal age over 35 years, preeclampsia or eclampsia, polyhydramnios, as well as a history of multiparity or previous abruption.
Finally, experiencing acute events like blunt trauma to the abdomen from a car crash or fall may increase the risk of placental abruption.
Most often, placental abruption presents with dark or bright red vaginal bleeding, which is accompanied by symptoms like abdominal pain over the area of the abruption, as well as back pain, particularly when the placenta is in a posterior location.
In addition, the uterus may contract and become rigid as it clamps down on the uterine vessels in an attempt to reduce the bleeding.
This can present as uterine tenderness and tetanic contractions, which last longer than 60 seconds.
Now, sometimes the bleeding can be concealed and trapped behind the placenta, which can delay the diagnosis and treatment.
If not promptly treated, extensive bleeding from placental abruption may lead to serious complications for both the mother and the fetus.
Maternal complications include hypovolemic shock, which can in turn cause renal failure, as well as Sheehan syndrome, which is a type of perinatal hypopituitarism.
Another possible complication is disseminated intravascular coagulation, or DIC, since the placenta is also rich in a procoagulant molecule called thromboplastin.
So, when the placenta detaches from the uterus, a large amount of thromboplastin is released, which causes widespread clotting. As a result, there’s consumption of coagulant factors, which ultimately causes more bleeding.
On the other hand, fetal complications include intrauterine hypoxia and asphyxia because the fetus is no longer receiving adequate placental perfusion. And finally there’s an increased risk of premature birth or fetal death.
Generally, diagnosis of placental abruption begins with history and physical examination. An ultrasound may show a retroplacental collection of blood which can support the diagnosis.
In addition, there can be decreased fetal movement and either fetal tachycardia or bradycardia, loss of variability, and presence of late decelerations.
In addition, blood tests usually show decreased levels of the clotting factor fibrinogen.
Finally, direct visualization of the placenta after delivery confirms the diagnosis of placental abruption.
Treatment of placental abruption depends heavily on the physiologic status of both the mother and the fetus, as well as the gestational age of the fetus.
The main approach involves giving intravenous fluids, blood products, and supplemental oxygen.
If the mother and fetus are stable, and the pregnancy is not past 36 weeks, then it’s recommended to monitor the pregnancy closely while the fetus develops.