Pneumothorax and hemothorax: Nursing
Pneumothorax and hemothorax: Nursing
Acute Final
Acute Final
Notes
| PNEUMOTHORAX AND HEMOTHORAX | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
| CAUSES AND RISK FACTORS |
| |
| PATHOPHYSIOLOGY |
| |
| SIGNS AND SYMPTOMS |
| |
| DIAGNOSIS |
| |
| TREATMENT |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
Transcript
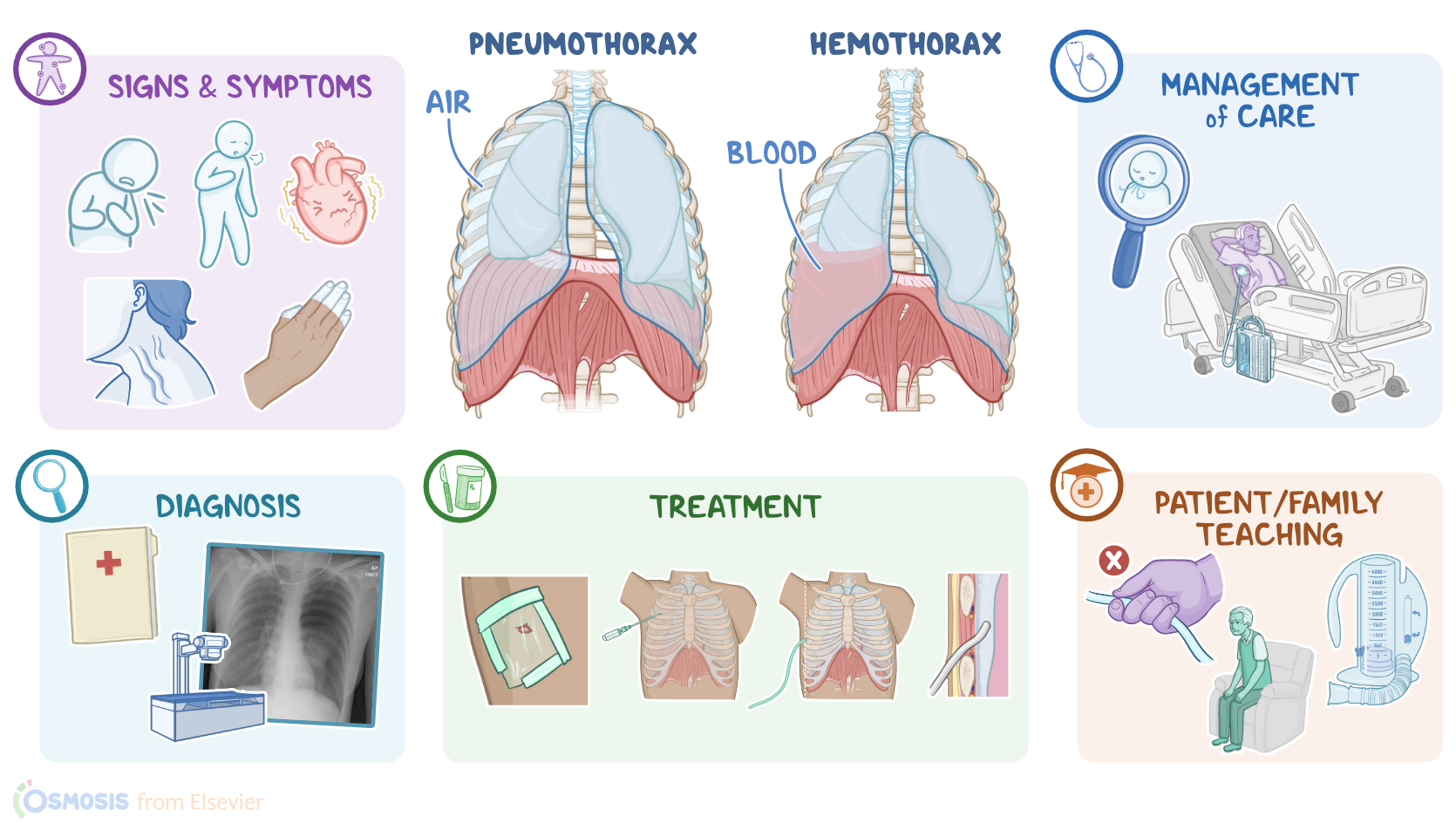
Pneumothorax and hemothorax are conditions that affect the pleural space surrounding the lungs. When air leaks into this space, it’s called a pneumothorax; whereas when blood fills this space, it’s called a hemothorax.
Now, let’s quickly review the anatomy and physiology of the pleural space. The lungs are lined with a membrane called the visceral pleura, while the chest cavity is lined with the parietal pleura. The thin space between these two membranes is called the pleural space. The pressure within the pleural space is negative, meaning it’s below atmospheric pressure. Now, the lung tissue’s elastic recoil applies a constant force that tries to contract the lungs, kind of like a stretched out rubber band. To prevent the lungs from shrinking, the negative pleural pressure around the lungs pulls the lung parenchyma outwards and counteracts the elastic recoil.
When a person inhales, the alveolar pressure becomes lower than the atmospheric pressure, which allows the air to enter the lungs. During exhalation, the alveolar pressure becomes greater than the atmospheric pressure, letting air move out of the lungs. However, at all times, the pleural pressure will remain lower than both the atmospheric pressure and the alveolar pressure, which helps prevent the lung from completely collapsing. Now, if pneumothorax or hemothorax occur, this physiological function of the pleural space gets disrupted.
Pneumothorax is categorized as either open or closed, depending on its cause. An open pneumothorax is caused by an opening in the chest wall that allows air to enter the pleural cavity from outside the body. A common type is traumatic pneumothorax due to a penetrating injury like a knife wound.
On the other hand, a closed pneumothorax results from an injury to the lungs that allows air to escape into the pleural space. This could be due to a traumatic cause, such as a broken rib from blunt damage piercing the lung, or an iatrogenic cause where a central venous line punctures the apical lung tissue during insertion.
Another example of a closed pneumothorax is spontaneous pneumothorax; this is usually caused by the rupture of pulmonary blebs, which are tiny air filled cysts on the lung’s surface. Both open and closed pneumothorax can cause life threatening tension pneumothorax. In either case, the damaged tissue forms a one way valve that lets air into the pleural space but prevents it from leaving.
Risk factors for pneumothorax include modifiable ones like smoking, chronic lung disease, previous pneumothorax, undergoing certain medical procedures like intubation and central venous line placement, and other nonmodifiable risk factors specific to spontaneous pnemothroax include tall and thin individuals who were assigned the male sex at birth.
When it comes to hemothorax, it is usually caused by blunt chest trauma that leads to bleeding into the pleural space. However, some medical procedures like subclavian vein catheterization, thoracic needle aspiration, and pleural or lung biopsy can damage the lung and nearby blood vessels causing both pneumothorax and hemothorax.
Okay, let’s look at what happens when air or blood fills the pleural space. Well, first, the negative pleural pressure becomes less negative or even positive, which means it’s less able to counteract the elastic recoil of the lungs. This causes the lung to shrink or even completely collapse if the pneumothorax or hemothorax is large enough.
Next, the accumulation of air or blood in the pleural space will keep the lung from expanding and decrease the vital capacity. In a tension pneumothorax, the one way valve keeps air from escaping so it accumulates quickly in the pleural space, causing it to balloon up. Eventually, it’ll start compressing the other organs in the mediastinum like the heart, leading to cardiovascular impairment, which is fatal if left untreated.
Additionally, with hemothorax, the blood that enters the pleural space is no longer in circulation, so it is considered as bleeding or blood loss. In a simple hemothorax, the blood loss is less than 1000 mL, while in a massive hemothorax, the blood loss is more than 1000 mL. Severe blood loss can cause a drop in blood pressure, potentially leading to circulatory shock, and sometimes death.
Signs and symptoms of a pneumothorax and hemothorax include dyspnea and mild tachycardia. Larger ones can cause dyspnea and respiratory distress, which presents as short, shallow, and rapid breathing. Additionally, hemothorax can cause hemodynamic instability. Tension pneumothorax is characterized by severe respiratory distress, distended neck veins, cyanosis, and hemodynamic instability.
During auscultation, there are reduced or absent breath sounds on the affected side. On percussion, there is hyperresonance with pneumothorax due to the presence of air within the pleural space, or dullness with hemothorax due to the presence of blood within the pleural space.
Diagnosis of both pneumothorax and hemothorax involves history and physical assessment, followed by a chest x-ray. For a pneumothorax, the affected lung will have a larger radiolucent, or darker space, when compared to the unaffected lung. For a hemothorax the blood will appear radiopaque. A large pneumo or hemothorax might show a collapsed lung, while a tension pneumothorax will also show displacement of the heart and trachea away from the affected side.
The treatment depends on the severity of the condition. Mild cases of spontaneous pneumothorax generally only need close monitoring. Open pneumothorax requires immediate vented dressing of the wound. This obstructs the wound and also acts like a one way valve that allows blood and air to drain out of the pleural space but prevents it from reentering.
When it comes to tension pneumothorax, the initial treatment to prevent air buildup is urgent needle decompression where a large bore needle is inserted into the 2nd intercostal space at the midclavicular line to release the trapped air. The definitive treatment for any type of pneumothorax and simple hemothorax is chest tube placement. However, massive hemothorax is treated by an open thoracostomy.
All right, when providing nursing care for a client who has pneumothorax or hemothorax, remember that their treatment will depend on the severity of their symptoms, but the main goal is to improve respiration and oxygenation.