Pulmonary edema: Nursing
Pulmonary edema: Nursing
NRS 428 WK 2: Respiratory
NRS 428 WK 2: Respiratory
Notes
| PULMONARY EDEMA | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
| CAUSES AND RISK FACTORS |
| |
| PATHOPHYSIOLOGY |
| |
| SIGNS AND SYMPTOMS |
| |
| DIAGNOSIS |
| |
| TREATMENT |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
Transcript
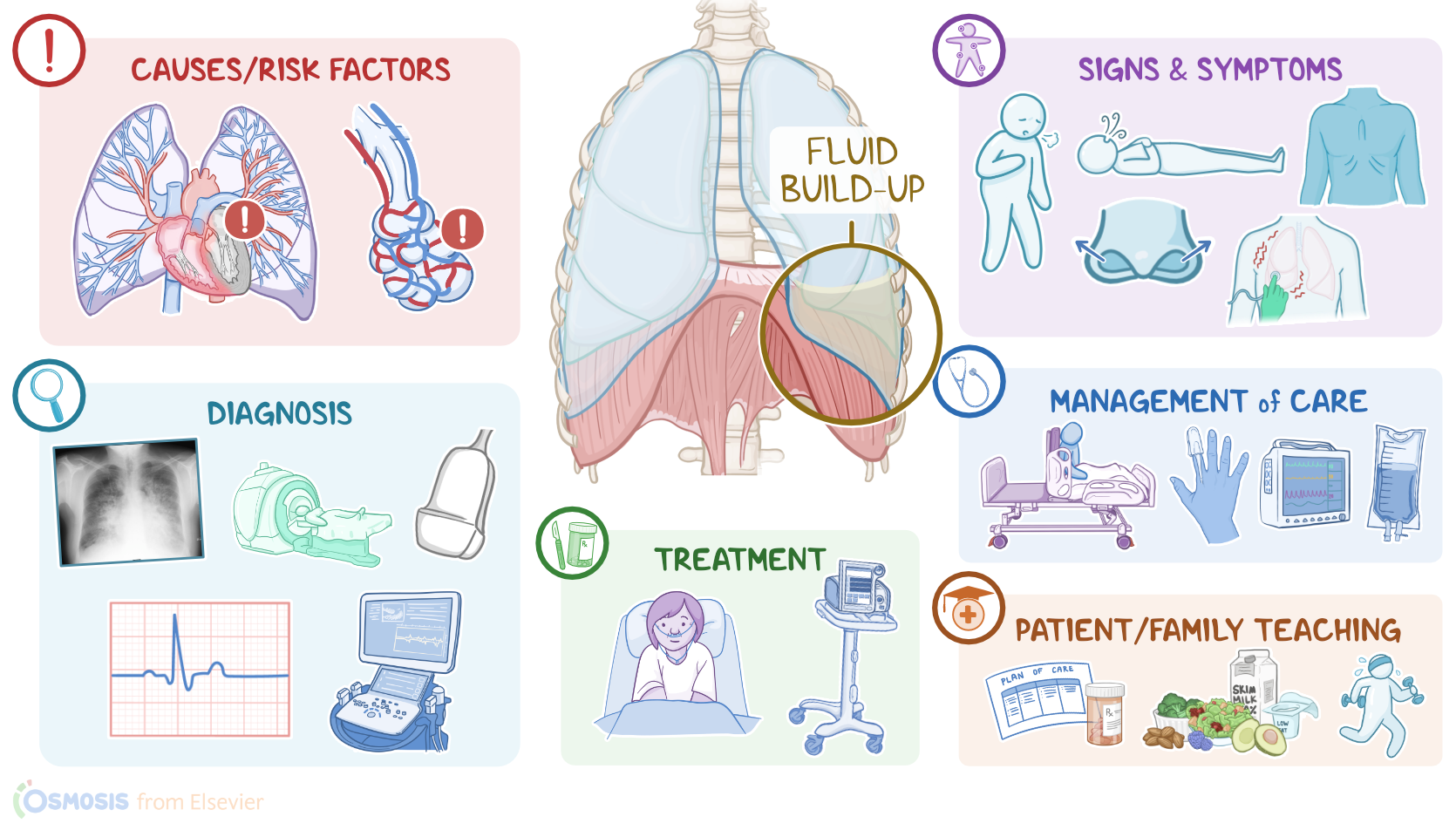
Pulmonary edema refers to the buildup of fluid in the lungs; and this can be further classified as cardiogenic pulmonary edema, which occurs as a result of heart disease; and noncardiogenic pulmonary edema, which usually occurs in the presence of damaged pulmonary capillaries.
To understand pulmonary edema, first, let’s quickly review the lower respiratory tract, which includes the lower part of the trachea, and the lungs containing the bronchi, bronchioles, alveolar ducts, and finally the alveoli. Alveoli are tiny air-filled sacs that are surrounded by tiny blood vessels, called capillaries.
Zooming in even more, we can see a tiny space between the alveolar wall and the capillary wall, called the interstitial space, which normally contains a small amount of interstitial fluid. And that’s where most gas exchange occurs.
So, each time we breathe in, the inhaled oxygen moves through the alveolar membrane, the interstitial space, and then through the capillary membrane to reach the blood, which is brought back through the pulmonary veins into the left heart and further into the systemic circulation.
On the other hand, carbon dioxide is carried from the right heart, through pulmonary arteries, into the lungs, where it diffuses from the capillaries through the interstitial space and into the alveoli, and then gets breathed out.
Now, cardiogenic pulmonary edema is caused by inadequate pumping of the heart, which usually occurs because of left-sided heart failure, ventricular arrhythmias, myocarditis, myocardial infarction, or valvular disorders, as well as severe hypertension and cardiomyopathy.
On the flip side, noncardiogenic pulmonary edema can be caused by damage to the lungs, which can occur because of pulmonary infections; acute respiratory distress syndrome, or ARDS for short; sepsis; pneumonia; as well as inhalation of toxic substances or aspiration of gastric contents. Other important conditions associated with noncardiogenic pulmonary edema include conditions that cause decreased circulating proteins, such as malnutrition, liver failure, and nephrotic syndrome.
Now, let’s switch our focus to pathology. With cardiogenic causes, such as left-sided heart failure, the left ventricle can’t pump blood effectively into the systemic circulation, meaning that blood starts to back up in the left atrium, and subsequently in the pulmonary veins and capillaries. The extra blood in the pulmonary capillaries results in increased pulmonary hydrostatic pressure.. Now, increased pressure within pulmonary capillaries pushes fluid into the interstitial space of the lungs, eventually causing pulmonary edema.
On the flip side, noncardiogenic causes like pneumonia are associated with an inflammatory process that makes nearby capillaries more permeable. As a result, proteins and fluid from the blood enter the interstitial space, leading to pulmonary edema.
Other noncardiogenic causes, such as nephrotic syndrome can cause pulmonary edema by decreasing protein production or increasing protein loss. Fewer blood proteins lower the oncotic pressure, and subsequently cause the shift of the fluid from the blood vessels into the interstitial space.
Now, once pulmonary edema occurs, that makes the gas exchange difficult because oxygen and carbon dioxide now have to diffuse through a wide layer of interstitial fluid to get from the alveoli to the capillaries. Less oxygen in the blood keeps tissues deprived of oxygen, which is known as hypoxia. Eventually, pulmonary edema can cause life-threatening complications, including respiratory failure.