Schizophrenia: Nursing
1,811views
Schizophrenia: Nursing
Watch later
Watch later
Notes
| SCHIZOPHRENIA | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
| CAUSES AND RISK FACTORS |
| |
| PATHOPHYSIOLOGY |
| |
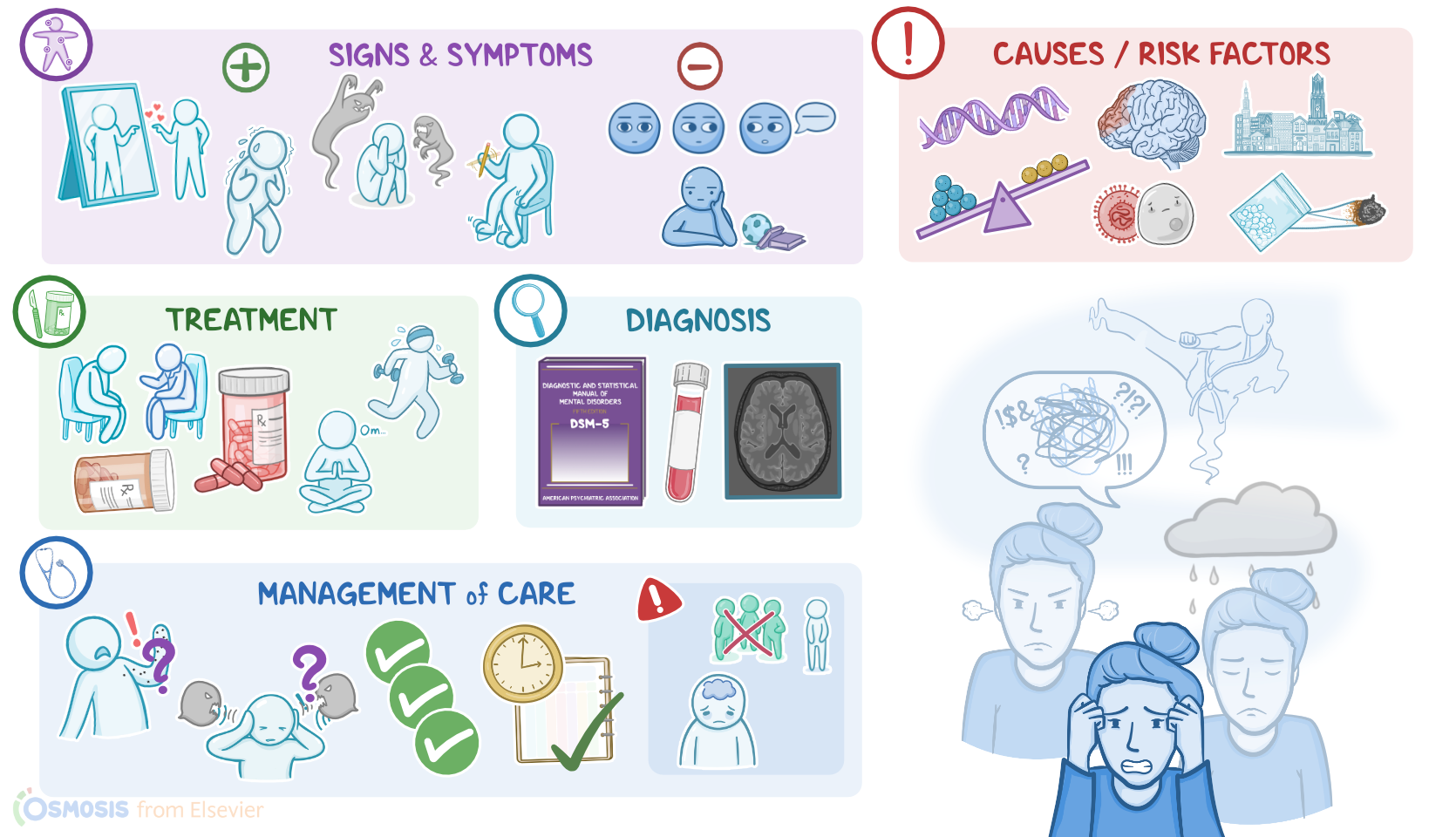
| SIGNS AND SYMPTOMS |
| |
| DIAGNOSIS |
| |
| TREATMENT |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
Transcript
Contributors
Schizophrenia is a psychiatric condition caused by imbalanced dopamine levels in the brain. It’s characterized by disturbances in perception, thinking, behavior, and emotions.
Alright, now let’s cover some basics of brain anatomy and physiology. Neurons communicate with each other through neurotransmitters.
Some, like glutamate, are excitatory neurotransmitters, meaning they cause neurons to fire. Some, like GABA, are inhibitory neurotransmitters and prevent a neuron from firing.
Finally, there are some like dopamine that could be excitatory or inhibitory depending on what neurons they act upon.
Dopamine is a neurotransmitter that’s primarily found in 4 main dopaminergic pathways of the brain; the mesolimbic pathway, which controls motivation and desire; the mesocortical pathway, which helps regulate emotions; the nigrostriatal pathway, which helps control voluntary movements; and lastly, the tuberoinfundibular pathway, which releases dopamine to limit the secretion of prolactin.
Now, the exact cause why schizophrenia occurs is still not fully understood; but, some theories suggest that it’s due to a combination of neurotransmitter imbalances in the brain, and anatomical brain changes due to genetic and environmental factors during early brain development.
Now, the main risk factors for developing schizophrenia include genetic predisposition, having a family history of schizophrenia; perinatal complications like infections, hypoxia, living in urban areas; as well as exposure to toxins; and the use of substances, especially cannabis, LSD, and methamphetamines.
Now, the mechanisms underlying the pathology of schizophrenia are poorly understood, but there seems to be abnormal levels of dopamine, particularly in the mesolimbic and mesocortical pathways. So, high levels of dopamine in the mesolimbic pathway result in positive symptoms, while low levels of dopamine in the mesocortical pathway cause negative symptoms.
Another contributor to the negative symptoms is the decreased activity of excitatory neurons throughout the brain that use glutamate as the neurotransmitter.
Finally, they are usually accompanied by specific anatomical changes like atrophy of the brain with reduced volume of the gray matter.
Now, moving on to clinical manifestations. Positive symptoms are those that occur “in addition” to normal experiences, therefore they are often referred to as “add-on” symptoms.
First, there are delusions, or strong false beliefs that the client might feel very strongly about even if there's strong evidence against it. For example, clients with persecutory delusions believe that they are going to be harmed or harassed by other people; while in grandiose delusions clients believe that they are famous or have unnatural superpowers.
Next up are hallucinations, or perceptions of something in the real world that’s not really present. The most common type of hallucinations are auditory hallucinations, which involve hearing voices. Less common are visual hallucinations, where clients see things that don’t exist; and tactile, olfactory, or gustatory hallucinations, when a person has a false perception of touch, smell, and taste.
Another important positive symptom is disorganized speech, which occurs because these individuals have difficulty controlling their flow of thoughts. As a result, they switch from one conversation topic to another one with no connection or associations.
Finally, there’s grossly disorganized or catatonic behavior, which can manifest as repetitive movements, unusual actions, bizarre posture, and not responding to other people's instructions.
On the flip side, negative symptoms represent the absence of normal behavior and the most characteristic ones are called flat affect and anhedonia. Flat affect manifests as decreased facial expressions, like frowning and smiling; reduced eye contact; and decreased speech intonation.
In addition, anhedonia is defined as the inability to enjoy pleasurable activities.
Finally, these clients may present with cognitive problems, such as the inability to focus, impaired memory, and decreased ability to solve problems; or mood symptoms, such as depression, anxiety, and suicidal ideations.
The diagnosis of schizophrenia is based on the client’s history and physical assessment. Diagnosis is confirmed using the Diagnostic and Statistical Manual for Mental Disorders fifth edition or DSM-5 criteria, which is a set of diagnostic criteria indicating the symptoms that must be present, and for how long, to diagnose a mental health condition.
Now, based on the DSM-5 criteria, schizophrenia is diagnosed in clients who present with at least two of the following symptoms over a one-month period: delusions, hallucinations, disorganized speech, disorganized or catatonic behavior, or negative symptoms.
But, it’s important to note that at least one of the symptoms has to be either delusions, hallucinations, or disorganized speech.
Besides the one-month period which is required to meet the criteria, another criterion is that some symptoms should stick around for at least six months, either before, when they’re called prodromal symptoms, or after, when they’re called residual symptoms.
Additionally, lab testing can be used to assess if the client is intoxicated; while imaging methods can be used to exclude the presence of tumors in the central nervous system, which could potentially cause similar symptoms.
Treatment of schizophrenia usually involves a combination of psychotherapy and pharmacotherapy. Psychotherapy, including cognitive-behavioral therapy, focuses on teaching the client strategies to challenge negative thoughts, feelings, and behavior patterns.
In addition, clients may benefit from lifestyle modifications like physical activity, yoga, meditation, deep-breathing exercises, and acupuncture.
Regarding pharmacotherapy, the first line medications are “atypical or second-generation” antipsychotics such as clozapine, risperidone, and olanzapine, which are better tolerated than the older “typical or first-generation” ones.
Finally, benzodiazepines might be administered to alleviate the anxiety some clients experience.
Okay, let’s talk about the nursing care you would provide for a client with schizophrenia. Your priority goals are to provide supportive care during symptom stabilization and maintain safety for the client and others.