Shock - Neurogenic: Nursing
Notes
| SHOCK - NEUROGENIC | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
| CAUSES AND RISK FACTORS |
| |
| PATHOPHYSIOLOGY |
| |
| SIGNS AND SYMPTOMS |
| |
| DIAGNOSIS |
| |
| TREATMENT |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
Transcript
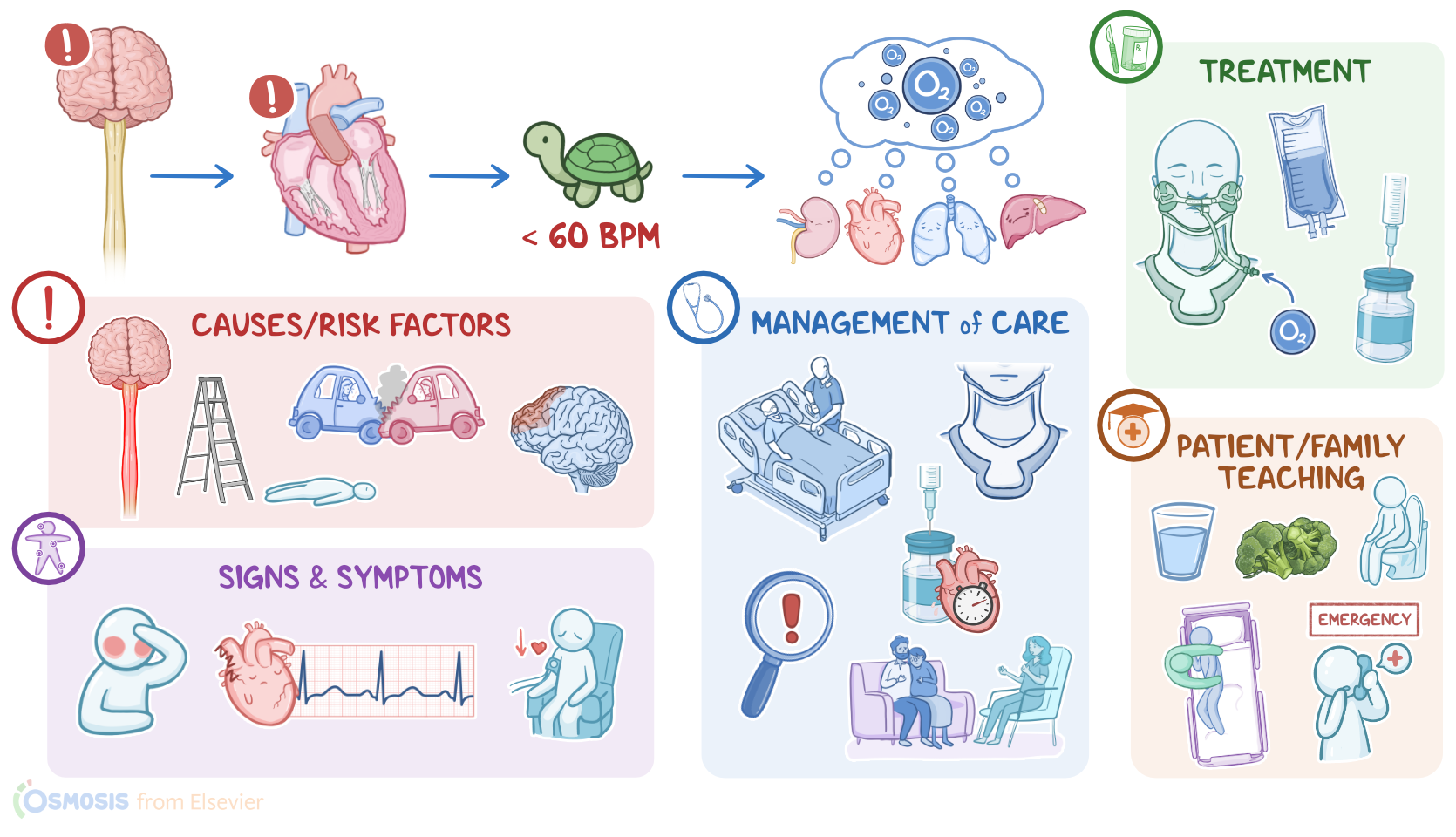
Shock is a life-threatening condition that occurs when the organs don’t receive enough oxygen and nutrients to function properly. Shock can be grouped into four types based on the cause: hypovolemic, cardiogenic, obstructive, and distributive shock. Neurogenic shock is a type of distributive shock where damage to the brain or spinal cord causes dysregulation of the cardiovascular system, leading to decreased heart rate and vasodilation, which eventually leads to impaired tissue perfusion.
Now, to understand the neurogenic shock, let’s quickly review the physiology of blood vessels, which contain smooth muscle in their walls. When the smooth muscle relaxes, it increases the diameter of blood vessels, called vasodilation. On the other hand, when smooth muscle contracts, the diameter of blood vessels decreases, called vasoconstriction.
The contraction and relaxation of smooth muscles are primarily controlled by the sympathetic nervous system, which normally maintains a partial constriction, generating enough force to keep blood moving through the circulatory system. The sympathetic system stimulation can increase or decrease to keep up with the body’s needs. Increased sympathetic stimulation of the blood vessels causes increased heart rate and vasoconstriction, which increases peripheral vascular resistance. Vasoconstriction, when the total blood volume is constant, raises blood pressure and allows blood to flow faster through the blood vessels. In contrast, decreased heart rate and vasodilation is typically caused by decreased sympathetic stimulation, in addition to inflammatory cytokines and histamine, which decrease peripheral vascular resistance. So, vasodilatation, when blood volume is constant, lowers the blood pressure and slows down the blood flow through the blood vessels.
Now let’s switch gears and look at the causes of neurogenic shock. This type of shock is primarily caused by trauma to cervical or upper thoracic segments of the spinal cord, which is typically associated with motor vehicle crashes, as well as severe falls, such as falling from a ladder. Other, less common causes include traumatic brain injury, Guillain-Barre syndrome, transverse myelitis, as well as spinal anesthesia.
Risk factors for developing neurogenic shock include anything increasing the risk of spinal cord trauma, such as engaging in high-risk behaviors, like speeding, and not wearing safety equipment when playing sports. Additionally, clients with a history of bone or joint disorders are also at a higher risk, since even minor trauma could damage the weakened bones, thereby injuring the spinal cord and potentially resulting in neurogenic shock.
The pathology behind neurogenic shock is based on the dysregulation between the sympathetic and parasympathetic stimulation of the cardiovascular system. Injury to the spinal cord can damage the neurons responsible for sympathetic innervation. As a result, the balance is tipped towards the parasympathetic system, causing bradycardia and massive peripheral vasodilation, causing blood to remain in the limbs instead of returning to the heart. All these factors together decrease the blood pressure and organ perfusion.
Now, most types of shock can be divided into four main stages: initial, compensatory, progressive, and refractory. But neurogenic shock deviates from this pattern. Things are pretty similar to other types of distributive shock during the initial stage, when systemic vasodilation causes less blood to return to the heart through the venous system; this, in turn, decreases cardiac output. As a consequence, body cells are not well-perfused, so they switch to anaerobic metabolism to produce energy, causing lactic acid to build up in the blood. When lactic acid builds up, that lowers blood pH, causing metabolic acidosis. Normally, this activates the compensatory stage, which involves stimulation of the sympathetic nervous system to increase the heart rate and vasoconstriction. However, in neurogenic shock, there’s a loss of the sympathetic activity, so the body fails to increase cardiac output. Therefore, with neurogenic shock, there’s no compensatory stage. If not managed in time neurogenic shock can progress to severe tissue hypoxia; and vital organs like the heart, brain, and kidneys may begin to shut down, leading to multiple organ failure.
Clinical manifestations of neurogenic shock share many similarities with other types of shock. There's hypotension, weak peripheral pulse and in severe cases, altered mental status or coma. Now, unlike with hypovolemic, obstructive, or cardiogenic shock, the skin can be warm and flush instead of cold and pale, and this is due to increased peripheral vasodilation. Furthermore, neurogenic shock is the only type of shock where there’s bradycardia instead of tachycardia since sympathetic regulation of the heart is impaired.
Spinal cord injury that causes neurogenic shock is often accompanied by other neurological symptoms. These include muscle weakness or paralysis, urinary incontinence, impaired respiration, and the inability to regulate temperature, where the client becomes poikilothermic, meaning they become dependent on the environment for temperature regulation.
Diagnosis of neurogenic shock starts with the client’s history and physical assessment and it’s made based on the symptoms and ruling out other causes of shock. This is followed by imaging tests like X-rays, CT scan, or MRI to look for the exact cause and location of the spinal cord or brain injury.
Finally, let’s take a look at treatment. The first step in the management of the client with neurogenic shock is to stabilize the client’s spine using a cervical collar, secure the airway, and provide oxygen. Some clients might also need mechanical ventilatory support. The management continues with early resuscitation with IV fluids and administration of vasoactive medications like norepinephrine. In the case of persistent bradycardia, atropine can be used to increase the heart rate. Finally, clients with neurogenic shock might benefit from the administration of corticosteroids, such as methylprednisolone. Finally, it’s important to address the underlying cause whenever possible, like performing spinal decompression procedures such as closed reduction using traction, or spinal surgery.