Shoulder dystocia: Nursing
Notes
| SHOULDER DYSTOCIA | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
| CAUSES AND RISK FACTORS |
| |
| PATHOPHYSIOLOGY |
| |
| SIGNS AND SYMPTOMS |
| |
| DIAGNOSIS |
| |
| TREATMENT |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
Transcript
Shoulder dystocia is an obstetrical emergency that can occur during vaginal delivery, and it refers to when the fetal shoulders can’t progress past the maternal pubic bone after the fetal head has been delivered. This usually requires additional obstetrical maneuvers to deliver the baby safely.
Let’s start by looking at the anatomy and physiology of the birth canal during delivery, starting with the pelvis, made up of the sacrum and the paired hip bones, each of which is made up of the ilium, ischium and pubic bones. The anatomy of the female bony pelvis differs from the male bony pelvis, in that it’s wider and flatter in shape and has a wide pubic arch, which helps with vaginal delivery. Usually, the female pelvic inlet is about 12cm in an antero-posterior diameter, and 13cm in a transverse diameter.
Now, remember that the bisacromial diameter, meaning the distance between the outermost parts of the fetal shoulders, is usually between 12 and 15 centimeters. Because of that, the fetal shoulders typically enter the pelvis at an oblique angle, and the posterior shoulder, meaning the one facing the back of the birth canal, is usually a little ahead. Following external rotation of the fetal head, the anterior shoulder can usually glide under the symphysis pubis in order to be delivered.
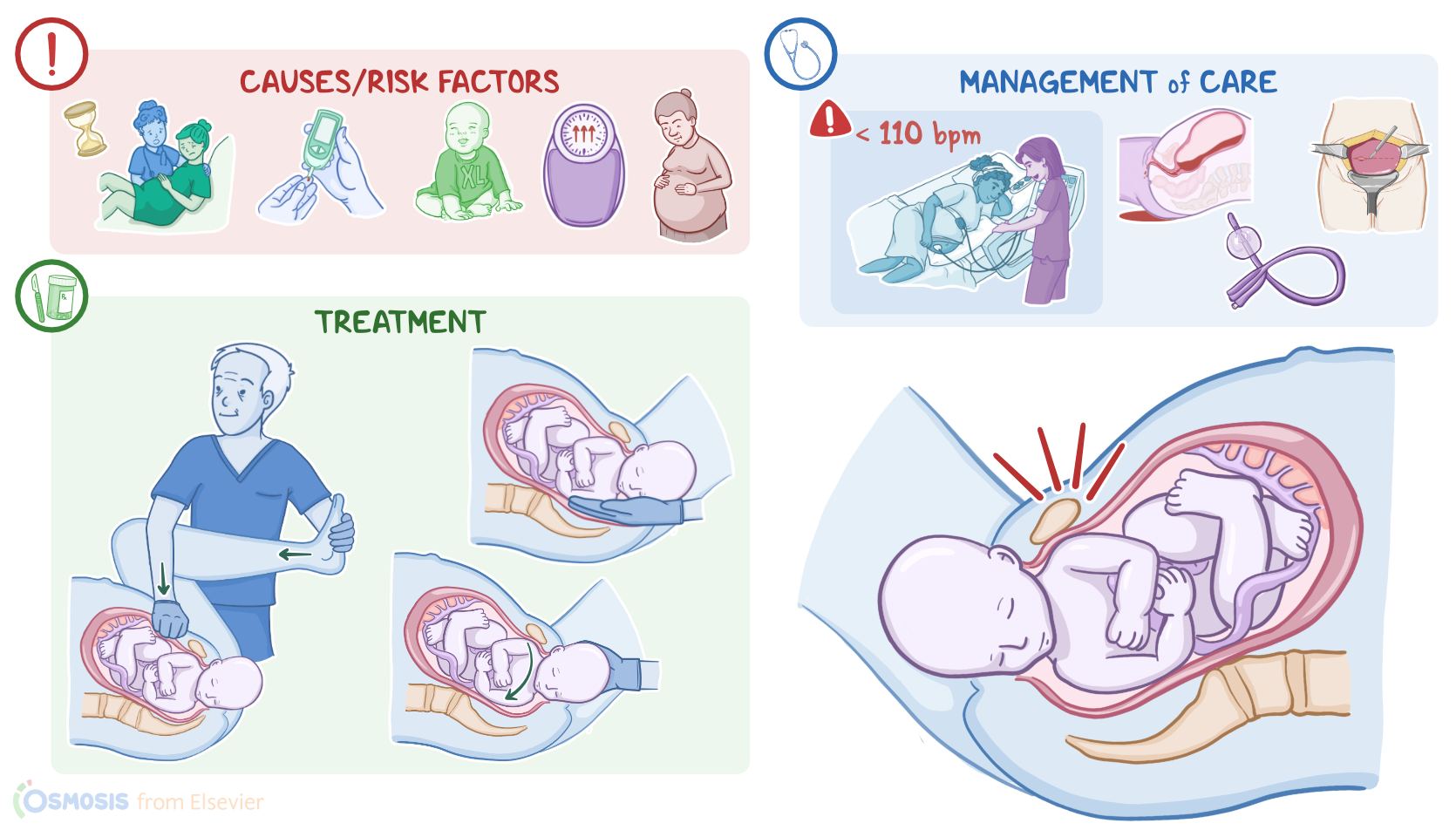
Now, shoulder dystocia is usually caused by discrepancy between fetal shoulders and maternal bony pelvis. So, risk factors for shoulder dystocia include maternal factors, which can be remembered with the acronym SAP-DOE. This stands for small pelvic inlet; advanced age; prior history of shoulder dystocia or large infants; gestational or pregestational diabetes, obesity, and excessive maternal weight gain. The main risk factor related to the fetus is fetal macrosomia, or a fetus that’s larger than normal. Finally, there are risk factors related to the labor process, which include a prolonged second stage of labor, abnormal labor progress, and labor induction. Now, pathology-wise, during delivery, the anterior fetal shoulder can become impacted behind the symphysis pubis or the posterior shoulder can be obstructed by the maternal sacrum bone.
Complications of shoulder dystocia can affect the mother, the fetus, or both. Maternal complications include postpartum hemorrhage, increased risk of perineal lacerations, sphincter injuries, and uterine rupture. Fetal complications include damage to fetal brachial plexus; umbilical cord compression and resulting hypoxia and acidosis; clavicular or humeral fractures; bruising and subdural hematomas; and even fetal death.
Clinically, one of the first signs of shoulder dystocia is known as the “turtle sign.” This is when after the head is delivered, it retracts back inside the birth canal, like a turtle’s head drawing into its shell. Another important red flag for shoulder dystocia is when the head to body delivery interval exceeds 60 seconds and the fetal shoulders haven’t been delivered using gentle downward traction movements.
Now, when it comes to diagnosis, while there are no clear-cut criteria for shoulder dystocia, the situation can be suspected if the turtle sign is present or there’s failure to deliver the fetal shoulders using basic routine maneuvers.
Treatment of shoulder dystocia includes first-line maneuvers, like the Mc-Roberts maneuver and suprapubic pressure. McRoberts maneuver is when the maternal thigh is hyper-flexed towards the abdomen, which straightens the maternal sacrum and lumbar spine. Suprapubic pressure is when pressure is applied to the suprapubic maternal area in a downward motion in order to decrease the fetal bisacromial diameter and dislodge the shoulder.
Second-line maneuvers include attempts to deliver the posterior arm and rotational maneuvers to try to reposition the fetal shoulders. If none of these maneuvers work, the fetal head can be slowly pushed back into the birth canal, and then a cesarean birth can be done.
Alright, let’s discuss the management of care for shoulder dystocia. Priority goals of nursing care include preventing maternal and fetal injury during delivery and providing emotinal support.
Now, when shoulder dystocia occurs during labor, take steps to prevent maternal and fetal injury. First, instruct your client to stop pushing. Then, call for assistance from the healthcare provider, as well as the neonatal team, and an additional nurse to ensure that there are enough team members to assist with maternal and fetal maneuvers, and to stabilize the newborn after delivery. Be sure to place a urinary catheter to drain your client’s bladder, which will decrease the risk of bladder trauma and allow more room for shoulder rotation.
Next, assist with maneuvers to safely deliver the fetus. Help your client to move toward the edge of the bed and closer to the healthcare provider, so there’s adequate room to accomplish the needed manipulations. Assist with the McRoberts maneuver with the help of another nurse, by grasping the thighs of each of your client’s legs and flexing them against the abdomen. If suprapubic pressure is also needed, apply direct pressure just above the mother’s symphysis pubis, and instruct the mother to push as pressure is applied. Remember that you should never apply fundal pressure over the uterus, because this can potentially worsen the problem and injure the mother or fetus.
During this time, closely monitor the fetal heart rate and pattern, and report to the healthcare provider if the fetal heart rate is less than 110 beats per minute or if late decelerations are present, and be ready to prepare your client for cesarean birth.
After delivery, assess the infant for signs of fractures, including crepitus, limb deformity, and bruising. Assess the mother for signs of birth trauma, like perineal tears; and be sure to institute frequent checks to ensure appropriate uterine involution and to look for complications such as postpartum hemorrhage. Finally, during your interventions, be sure to calmly reassure your client by providing clear explanations of interventions.
Okay, let’s move on to some teaching. First, explain that shoulder dystocia is an emergency situation where their baby’s shoulders get stuck on their pubic bone. Describe each maneuver that was used to safely deliver their baby.
After their baby is delivered, let them know that both they and their baby will be checked frequently to ensure proper identification and management of complications. Lastly, talk about the increased risk of shoulder dystocia with subsequent pregnancies, and discuss ways to decrease the risk through weight and glucose control.
Alright, as a quick recap… Shoulder dystocia is an emergency which occurs during vaginal delivery when the fetal shoulders become lodged behind the mother’s pubic bone. This usually requires additional obstetrical maneuvers in order for the baby to be safely delivered. Shoulder dystocia is sometimes unpredictable and unpreventable, but there are maternal, fetal, and procedural factors that increase risk. During delivery, shoulder dystocia is often diagnosed with the “turtle sign” where the fetal head retracts back into the birth canal.
First-line maneuvers include McRoberts maneuver and suprapubic pressure. Other maneuvers include delivery of the posterior arm and rotational maneuvers to try to reposition the fetal shoulders. If none of these work, the fetal head can be slowly pushed back into the birth canal, and then a cesarean birth can be done. Goals of nursing care include preventing maternal and fetal injury during delivery and providing emotinal support. General client and family teaching focuses on understanding shoulder dystocia, its risk factors, and how it is managed.
Key Takeaways
Shoulder dystocia is a birth complication that occurs when the baby's shoulder becomes stuck behind the mother's pubic bone during delivery. This can cause the baby to become lodged in the birth canal and can prevent the baby from being born safely.
Shoulder dystocia is sometimes unpredictable and unpreventable, but there are maternal, fetal, and procedural factors that increase risk. During delivery, shoulder dystocia is often diagnosed with the turtle sign � where the fetal head retracts back into the birth canal.
Management usually requires additional obstetrical maneuvers, such as McRoberts and posterior arm and rotational maneuvers, in order for the baby to be safely delivered. When such maneuvers fail, then a cesarean birth might be the best option. Goals of nursing care during shoulder dystocia include preventing maternal and fetal injury and providing emotional support