Small for gestational age (SGA) infant: Nursing
Notes
| SMALL FOR GESTATIONAL AGE INFANT (SGA) | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
| CAUSES AND RISK FACTORS |
| |
| PATHOPHYSIOLOGY |
| |
| SIGNS AND SYMPTOMS |
| |
| DIAGNOSIS |
| |
| TREATMENT |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
Transcript
Small for gestational age or SGA for short, is a term used to describe an infant whose weight is below the 10th percentile for gestational age. In other words, this is an infant who weighs less than 90% of infants of the same gestational age.
SGA infants can be born prematurely, at term, or at post term, and they may also have experienced intrauterine growth restriction, or IUGR for short. It’s important to note, though, that not all IUGR infants end up being SGA.
Now, first, let’s cover some basic physiology. Gestation refers to the period between conception and birth, which typically lasts for 40 weeks. During these 40 weeks, the embryo, and later fetus, grows and develops within the uterus. On the other hand, gestational age is a term used to describe a newborn based on their physical and neuromuscular characteristics.
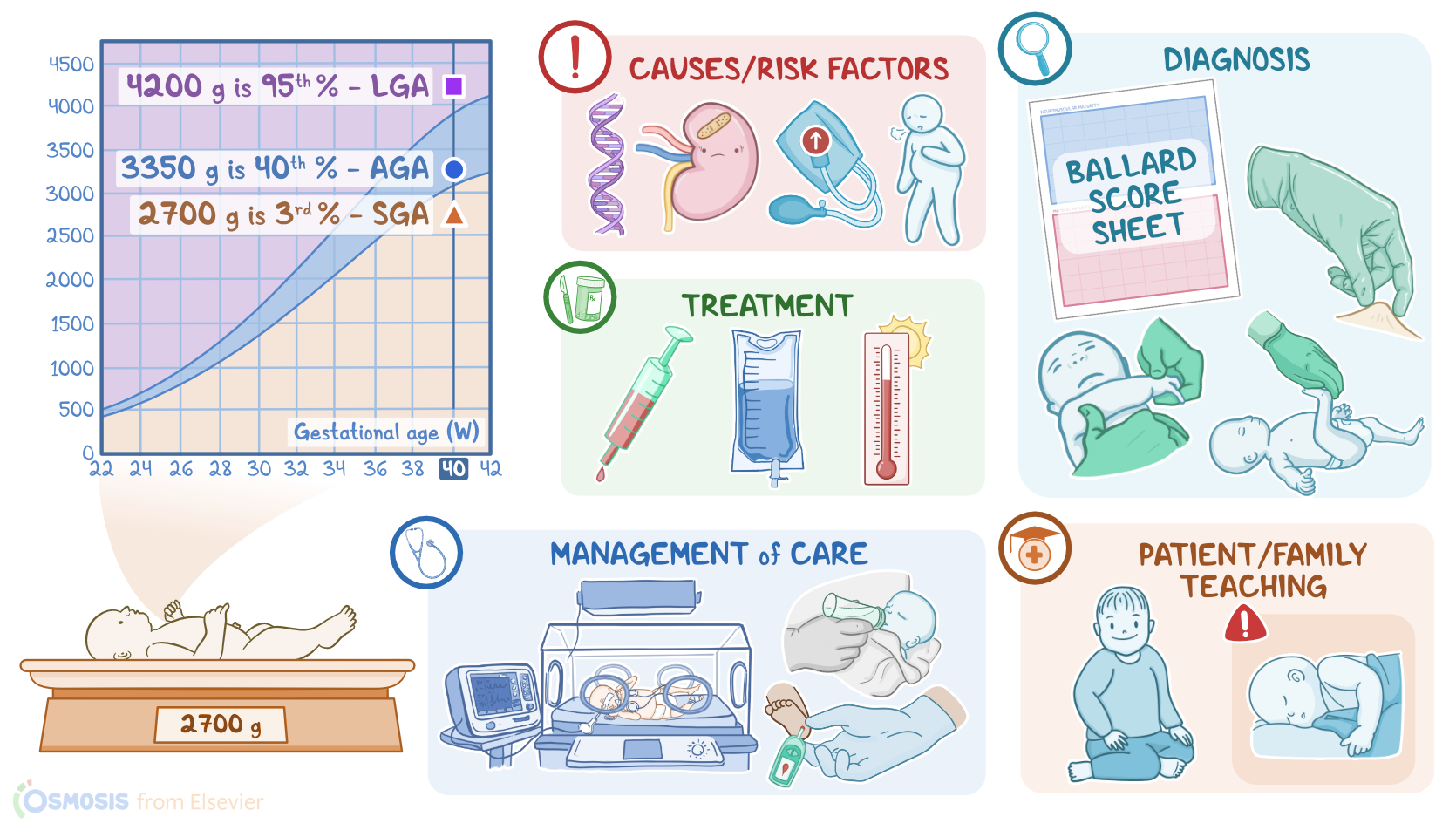
Now, based on the gestational age and the infant’s birth weight, we can determine birth weight percentiles. The birth weight percentile helps us evaluate the infant’s intrauterine growth and development, which is considered normal when the value is between the 10th and 90th percentile.
For example, an infant weighing around 3350 grams is within the 40th percentile, and is considered appropriate for gestational age, or AGA. On the other hand, an infant weighing around 2700 grams is within the 3rd percentile, and therefore SGA. Finally, an infant weighing around 4200 grams is within the 95th percentile and is considered large for gestational age, or LGA for short.
Now, moving on to causes. Some SGA infants can be genetically predisposed to be physiologically small; while others can have impaired fetal development due to some other fetal or maternal condition.
Now, factors that increase the risk of impaired fetal development can be classified as fetal or maternal. Starting with fetal risk factors, these include genetic abnormalities, multiple gestation, as well as congenital infections, which are grouped under the acronym TORCH. T stands for Toxoplasmosis, O for Other infections like Syphilis, R for Rubella, C for Cytomegalovirus, and H for Herpes Simplex. Next up are maternal factors that include hypertension, diabetes, asthma, renal disease, poor nutrition or insufficient weight gain during pregnancy, and maternal exposure to substances that are harmful to the fetus, like cigarette smoke or illicit drugs.
Alright, let’s switch our focus to pathology. When conditions cause the fetus to receive inadequate oxygen, glucose, and other nutrients necessary for growth, the infant can experience IUGR. If there’s impaired fetal development during the early stages of gestation, which is a time when rapid cell proliferation takes place, all parts of the fetus are affected proportionally, eventually causing symmetrical IUGR, meaning that weight, length, and head circumference plot similarly on a growth curve.
On the other hand, asymmetrical IUGR usually occurs when fetal development is impaired during the later stages of gestation, which is a time when there’s rapid cell proliferation in addition to an increase in cell size. So, in asymmetrical IUGR, the fetus redirects blood from less vital organs, like the spleen, liver, and adrenal glands, to vital organs, like the brain and heart, so the head size and length are spared, but the infant’s organ size and weight are decreased.
Now, SGA infants are more likely to develop several complications, including perinatal asphyxia, meconium aspiration, respiratory distress, impaired immune function, hypoglycemia, polycythemia, and jaundice. Finally, there is frequently an increased risk of preterm labor, leading to a series of complications associated with prematurity.
In terms of clinical manifestations, SGA infants typically present with decreased subcutaneous fat and muscle mass. Their skin is often loose and dry, with decreased turgor, and they may have a ruddy appearance if polycythemia is present. They may also have low or flaccid muscle tone. Now, symmetrical IUGR infants have a proportionally small size, meaning their head, chest, and length measurements are all below normal. In contrast, infants with asymmetrical IUGR have a normal head circumference, a large head-to-body ratio, and normal length.
Diagnosis is based on the assessment of gestational age, which can be made prenatally, meaning before birth, or postnatally, meaning after birth. Prenatal gestational age is determined by the length of pregnancy after the first day of the mother’s last menstrual period, expressed in weeks and days. Additionally, an ultrasound can be used to evaluate the fetal size and weight.
On the other hand, postnatal gestational age is primarily assessed using the New Ballard Score, which assesses the infant’s maturity rating by evaluating physical and neuromuscular characteristics.
Treatment primarily focuses on managing possible complications. Hypoglycemia may require IV glucose administration; infections can be treated with antimicrobials. It’s also important to ensure proper environmental temperature to prevent further heat loss.
Okay, now let’s talk about the nursing care you’ll be giving to an SGA infant. Your priority nursing goals are to support thermoregulation and monitor for complications. Begin by ensuring the infant is in a neutral thermal environment. Place the infant under a radiant warmer or in an isolette, and closely monitor them until their temperature has stabilized. Next, monitor the infant for complications. Institute pulse oximetry monitoring and assess their respiratory status.
Key Takeaways
Small for gestational age or SGA is a medical term used to describe a neonate with a birth weight below the 10th percentile of gestational age and at great risk of complications. Risk factors include genetic abnormalities, multiple gestations, intrauterine growth restriction, as well as congenital infections, which are grouped under the acronym TORCH.
SGA can also be due to maternal hypertension, maternal diabetes, maternal asthma, or other maternal conditions like renal disease, poor nutrition or insufficient weight gain during pregnancy, and maternal exposure to harmful substances like illicit drugs during pregnancy.
SGA infants are at a higher risk for certain complications like respiratory distress, poor thermoregulation, hypoglycemia, and polycythemia. Nursing care goals include supporting thermoregulation and monitoring for complications. Teaching should center on explaining the condition, caring for the baby at home, promoting healthy pregnancies in the future, and when to seek medical care.