Urinary incontinence - Stress: Nursing process (ADPIE)
1,361views
Urinary incontinence - Stress: Nursing process (ADPIE)
Watch later
Watch later
Notes
| URINARY INCONTINENCE - STRESS | ||
| KEY POINTS | NOTES | |
| PATIENT REPORT |
| |
| PATHOPHYSIOLOGY |
| |
| DIAGNOSIS AND TREATMENT |
| |
| ASSESSMENT |
| |
| NURSING DIAGNOSES |
| |
| PLANNING |
| |
| IMPLEMENTATION |
| |
| EVALUATION |
| |
Transcript
Heidi Anderson is a 60-year-old female who presents to her primary care clinic with reports of urine leakage when she sneezes, coughs and during exercise.
Her symptoms started one year ago, and she started wearing a panty liner which she changes several times each day.
Mrs. Anderson has had two vaginal births and one cesarean section. She has been very embarrassed about her incontinence and has finally gathered the courage to seek treatment.
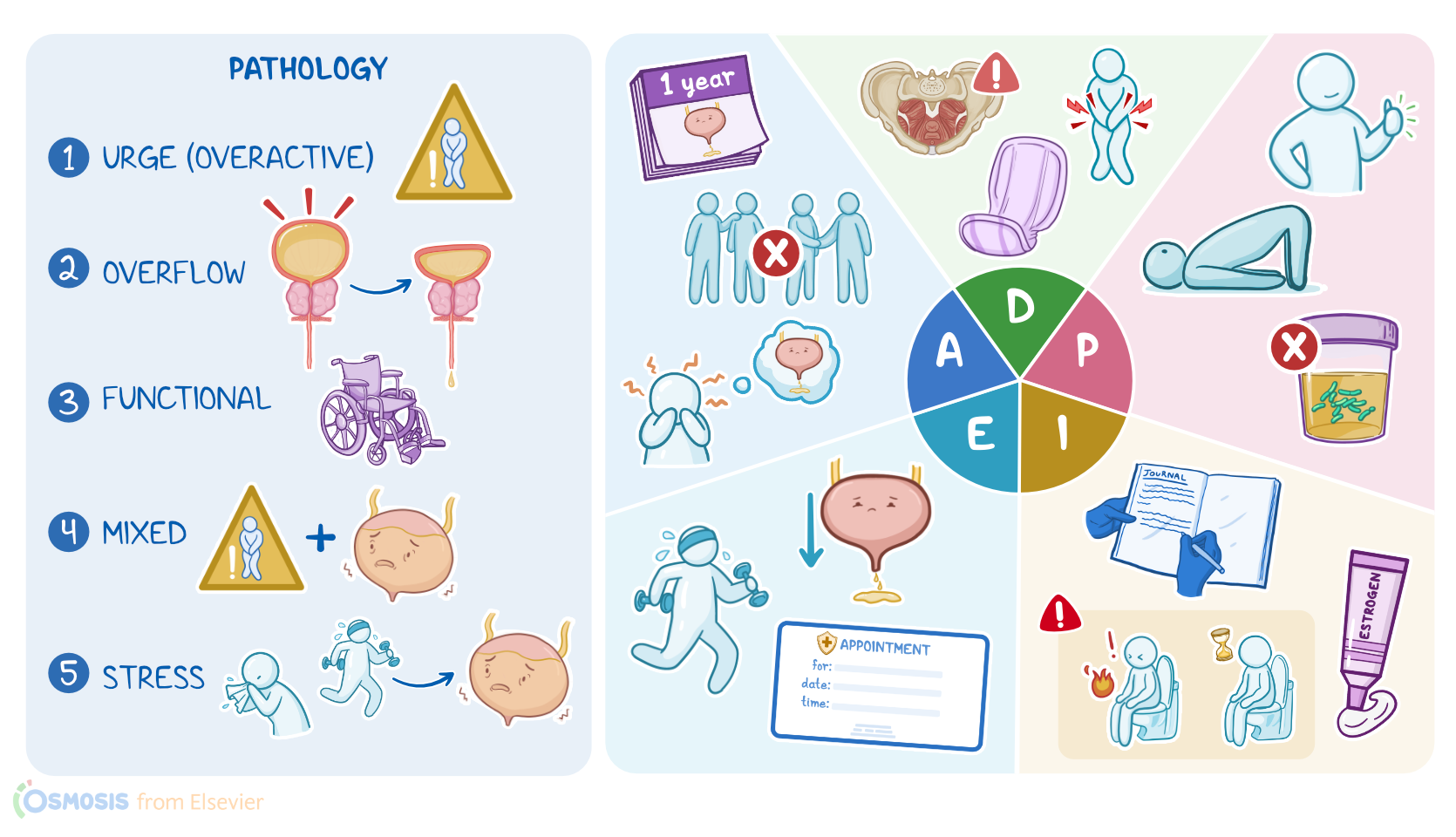
Urinary incontinence is the loss of bladder control, meaning that urine leaks involuntarily, causing both social and hygienic problems.
There are five major types of urinary incontinence. So, when there is a sudden urge to urinate that is difficult to delay, that’s urge incontinence, also known as an overactive bladder.
Overflow incontinence occurs when the pressure from a bladder that gets too full causes urine to leak out.
This can be caused by problems associated with urinary retention like spinal cord injuries or an enlarged prostate.
Functional incontinence happens when either a physical, cognitive, or environmental problem makes it hard to reach the bathroom in time, like with mobility problems or dementia.
There is also a type of mixed incontinence, which is a combination of two or more types of incontinence, usually urge incontinence and stress incontinence.
Stress incontinence is the most common type of incontinence. It occurs when urine leaks out because of increased intraabdominal pressure, like when coughing, sneezing, laughing, and during physical exercise.
Stress incontinence is usually caused by weakened pelvic floor muscles, which are a group of muscles that support the bladder, uterus, vagina, and bowel.
Pregnancy and childbirth are the most common causes of a weakened pelvic floor, especially with multiple pregnancies or trauma caused by vaginal deliveries assisted by instruments like forceps.
The risk also increases during menopause because decreased estrogen causes atrophy of pelvic tissue.
Complications of stress incontinence include decreased quality of life and social anxiety from fear of leaking urine.
The risk for urinary tract infections is also increased, as well as the possibility of skin breakdown can occur from a moist environment.
The diagnosis of stress incontinence is based on the client’s history and physical examination.
A bladder stress test, also called a cough stress test, consists of observing urine loss from the bladder when the client coughs or bears down.
Pelvic floor muscle strength can be determined by a vaginal digital exam. Initial treatment of stress incontinence includes pelvic floor strength training which will include learning how to do Kegel exercises, where the pelvic floor muscles are repeatedly tightened, held for a few seconds, and then relaxed.
The client can also be taught to quickly contract their pelvic floor muscles just before an activity that normally causes urine leakage.
In postmenopausal women, intravaginal estrogen cream can help reduce atrophy of pelvic floor tissues.
Other treatments include mechanical devices such as intravaginal pessaries that provide support to the bladder neck.
If the client is overweight, weight loss can be helpful in reducing intra-abdominal pressure.
When other interventions are unsuccessful, surgical options include procedures aimed at stabilizing the urethra and bladder to help them be more resistant to intra-abdominal pressure.
Okay, now that we understand stress incontinence, let’s get back to assess our client, Mrs. Anderson.
You enter her room, introduce yourself, perform hand hygiene, and confirm her identity. You begin by asking when her urinary incontinence started, and she tells you that it has been happening for about 1 year.
Key Takeaways
Stress urinary incontinence (SUI) is a type of urinary incontinence that occurs when urine leaks out because of increased intraabdominal pressure, like when coughing, sneezing, laughing, and during physical exercise. Stress incontinence is usually a result of weakened pelvic floor muscles, which are a group of muscles that support the bladder, uterus, vagina, and bowel. Pregnancy and childbirth are the most common causes of a weakened pelvic floor, especially with multiple pregnancies or trauma caused by vaginal deliveries assisted by instruments like forceps. Treatment options may include lifestyle changes, pelvic floor exercises (Kegel exercises), medical devices, medications, or surgery in severe cases.
Sources
- "Increased risk of stress urinary incontinence surgery after hysterectomy for benign indication-a population-based cohort study" Am J Obstet Gynecol (2023)
- "The pathophysiology of stress urinary incontinence: a systematic review and meta-analysis" Int Urogynecol J (2021)
- "A levator ani midurethral support via single vaginal incision technique to treat stress urinary incontinence: A case report" Case Rep Womens Health (2023)
- "Harrison’s Principles of Internal Medicine, 21st edition" McGraw Hill / Medical (2022)
- "Critical Care Nursing: Diagnosis and Management, 9th edition" Elsevier (2021)
- "Health Assessment for Nursing Practice, 7th edition" Elsevier (2021)
- "Electromyographic Biofeedback for Stress Urinary Incontinence or Pelvic Floor Dysfunction in Women: A Systematic Review and Meta-Analysis" Adv Ther (2021)