Peripheral venous disease (PVD): Nursing process (ADPIE)
Peripheral venous disease (PVD): Nursing process (ADPIE)
Week 10 modules
Week 10 modules
Notas
| PERIPHERAL VENOUS DISEASE (PVD) | ||
| KEY POINTS | NOTES | |
| PATIENT REPORT |
| |
| PATHOPHYSIOLOGY |
| |
| DIAGNOSIS AND TREATMENT |
| |
| ASSESSMENT |
| |
| NURSING DIAGNOSES |
| |
| PLANNING |
| |
| IMPLEMENTATION |
| |
| EVALUATION |
| |
Transcripción
Muriel Diallo is a 45-year-old female client with a history of peripheral venous disease and obesity. She is referred to the vein clinic by her primary care provider for treatment of a chronic, non-healing leg ulcer in her right lower extremity.
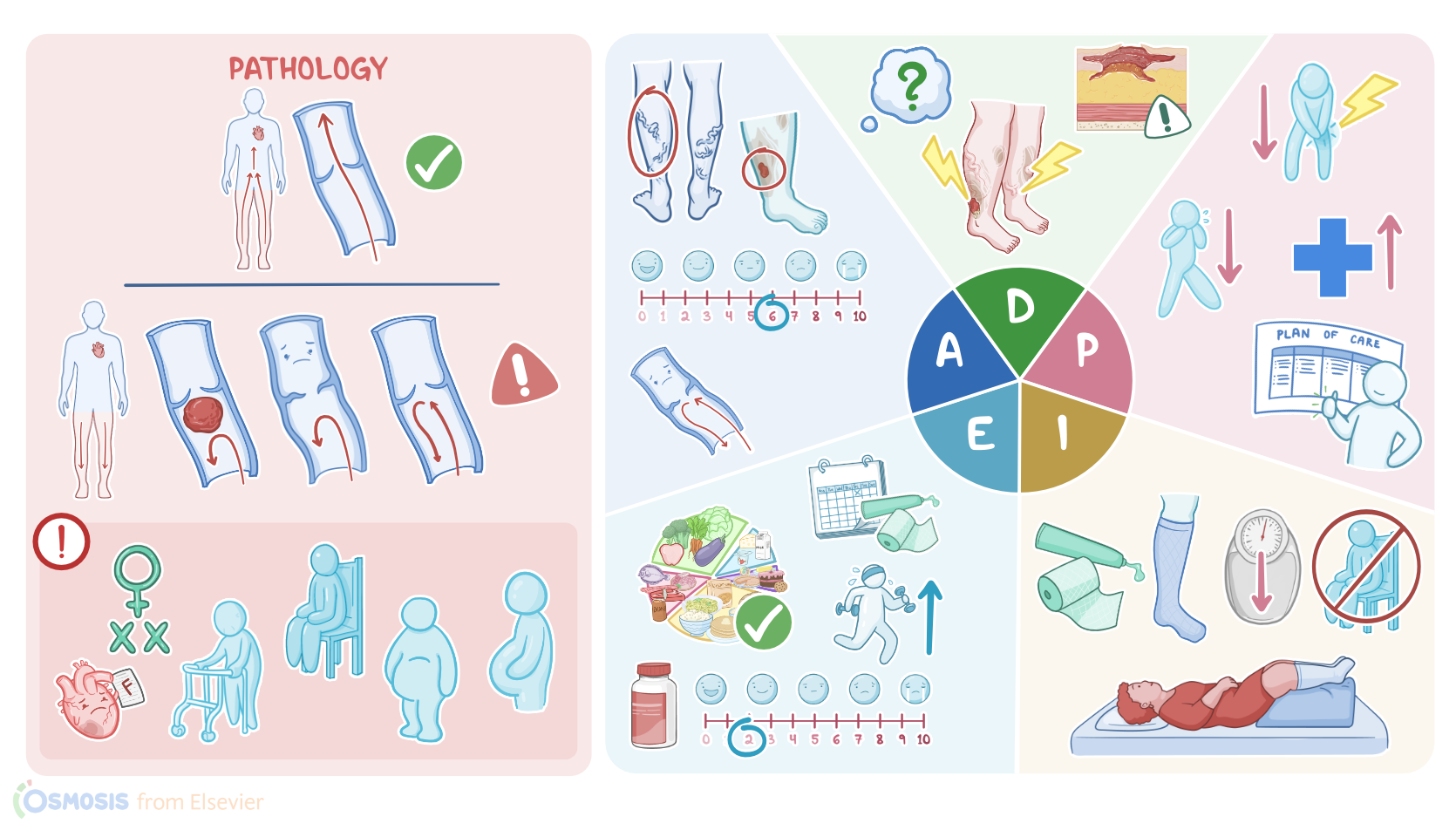
Peripheral venous disease, or PVD for short, is characterized by an obstruction or defect of the veins, and most often affects the legs. Normally, veins drain blood from peripheral organs and tissues towards the heart, and they have one-way valves to prevent backflow.
In PVD, veins are either obstructed by a blood clot or embolus, are weak or dilated, or there’s valvular insufficiency, so blood ends up leaking backward and pooling in the lower legs, leading to venous hypertension.
Risk factors for PVD include female sex, increasing age, sedentary lifestyle, obesity, and pregnancy. Other important risk factors for PVD include associated conditions like heart failure, varicose veins, and having a history of trauma or surgery.
Finally, another risk factor for PVD involves standing or sitting with the legs crossed for long periods of time. Okay, now clients with PVD often report pain in the legs, swelling, and a sensation of heaviness.
Fluid and red blood cells can leak out of the small veins and capillaries and into the surrounding tissues, causing edema and inflammation in the lower extremities. As the red blood cells break down in the tissue, they release hemosiderin, which eventually causes the skin to take on a brownish discoloration.
Moreover, as normal subcutaneous tissue is replaced by fibrous tissue, the skin becomes thick, leathery, and itchy. This will cause the skin to become more vulnerable to ulceration and painful sores, most often above the medial malleolus.
Clients with PVD may also develop some serious complications. First off, clients may develop chronic non-healing sores and ulcers, which pose a risk for infection and pain.
In addition, pooling of blood can increase the risk of blood clots formation within the veins which can cause inflammation and thrombophlebitis. Diagnosis of PVD relies largely on the client’s history and physical examination.
In addition, a venous ultrasound is usually performed to visualize venous blood flow and determine the presence of a blood clot. Alternatively, a venography procedure can be performed by injecting a dye into the veins, and an X-ray is taken to identify any obstruction.
When DVT or pulmonary embolism are suspected, a blood test should be performed to measure the D-dimer, which is a break-down product from blood clots.
Treatment options for PVD include increasing activity, elevating the legs above the heart, as well as application of compression stockings or tubular support bandages to help prevent backflow of blood, promoting venous return upward toward the heart.
Rarely, surgical treatment is required, such as a vein transplant, repair, or removal. You begin your assessment by asking how Mrs. Diallo is feeling. She tells you the sore on her leg is painful and that lately her legs have been more swollen and have felt heavy.
Her vital signs are heart rate 80 beats per minute and regular; respiratory rate 16 breaths per minute with clear breath sounds bilaterally; blood pressure 122/80 mmHg; temperature 97.9° F or 36.6°C; pain 6/10 located on her right leg.
As you assess her lower extremities you note the following: posterior tibial and pedal pulses are 2+; the skin on her lower extremities is dry,flaky, and leathery with a brownish discoloration; edema is 3+.
You notice bulging rope-like veins bilaterally. There is an open ulcer with irregular borders located between the right lateral malleolus and calf muscle. There is a moderate amount of thick exudate present on the wound.
You review the results of her venous ultrasound which shows vein dilation, valvular incompetence, and varicosities. ABI results for right and left legs are 1.0 and 1.2 respectively.
Fuentes
- "Harrison’s Principles of Internal Medicine, 21st edition" McGraw Hill / Medical (2022)
- "Pathologic Disparities Between Peripheral Artery Disease and Coronary Artery Disease" Arterioscler Thromb Vasc Biol (2020)
- "Heart Disease and Stroke Statistics-2022 Update: A Report from the American Heart Association" Circulation (2022)
- "Clinically-indicated replacement versus routine replacement of peripheral venous catheters" Cochrane Database Syst Rev (2019)
- "Health Assessment for Nursing Practice, 7th edition" Elsevier (2021)
- "Critical Care Nursing: Diagnosis and Management, 9th edition" Elsevier (2021)
- "Symptoms in Dilating Venous Disease" Curr Cardiol Rev (2020)