

When you picture a 19th-century physician, do you imagine a black leather medical bag swinging at their side as they brave a stormy night, armed with little more than a stethoscope, keen observation, and clinical judgment? This pervasive image captures the origins of internal medicine, a specialty born from careful listening, thoughtful examination, and relentless curiosity.
Derived from the German concept of Innere Medizin, internal medicine is a medical specialty in which internists diagnose, treat, and coordinate care for adult patients with complex, chronic, and multisystem diseases, emphasizing whole-patient care rather than surgical or single-organ intervention. Without strong internal medicine leadership, healthcare systems face greater care fragmentation, delayed diagnoses, inefficient resource use, and poorer outcomes for patients with complex, chronic, and multisystem diseases.
Internal medicine emerged as a discipline dedicated to understanding diseases of the body’s internal organs. Today, internal medicine stands as a cornerstone of modern healthcare, with internists serving as expert diagnosticians who manage complex, multisystem disease. From diabetes and heart failure to cancer and autoimmune disorders, internists are trained to see the whole patient rather than a single symptom, with clarity and precision.
From candlelit bedside exams to clinics equipped with AI-driven diagnostics, internal medicine has evolved into a specialty that blends cutting-edge science with the art of listening to achieve compassionate, patient-centered care. To understand how it reached this point, let’s take a few minutes to learn to trace the history of internal medicine, spotlighting the pioneers and breakthroughs that shaped the field.
Origins of Internal Medicine: The Rise of Innere Medizin
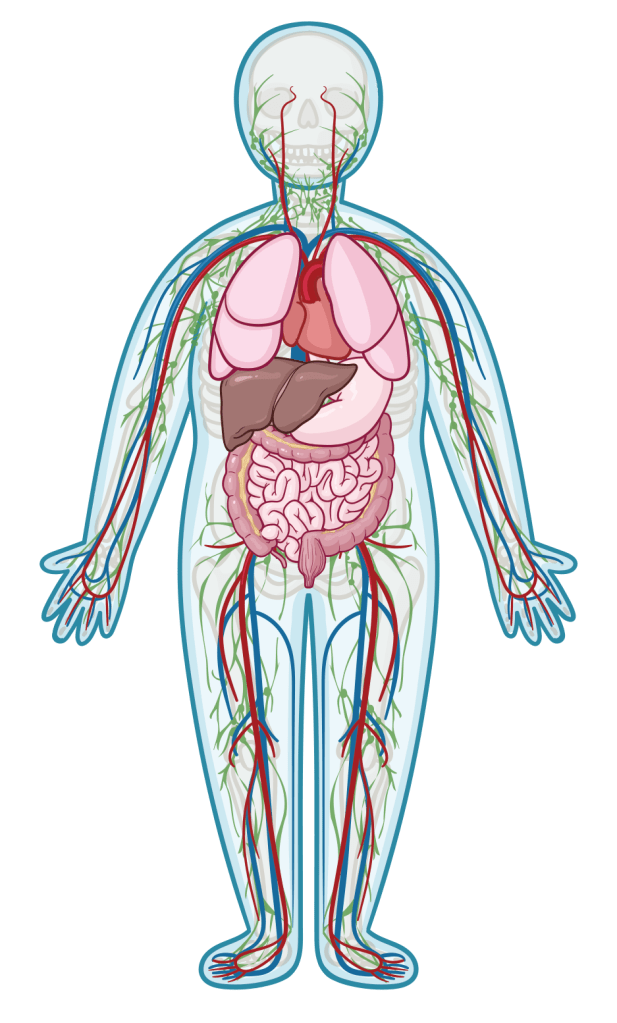
In 19th-century Europe, medicine relied heavily on observation and intuition. In Germany, the concept of Innere Medizin (internal medicine) transformed clinical practice by focusing on diseases of hidden, internal organs such as the heart, lungs, liver, and kidneys. Unlike surgery or obstetrics, this new approach sought to explain illness through the systematic analysis of hidden physiological processes such as tuberculosis, heart disease, and kidney failure.
Johann Lukas Schonlein, a German physician with rock-star charisma, led the charge. Teaching in Wurzburg and later Berlin, he dragged students to the bedside, insisting they learn from patients, not dusty textbooks. He’d point to a patient’s flushed cheeks, swollen belly, or rapid pulse, and urge his pupils to listen closely. A fever could mean typhoid, tuberculosis, or a heart infection. Schonlein taught doctors to be detectives, piecing together clues from breath, history, and physical signs. His clinics were like medical theaters. Students watched him palpate an abdomen for an enlarged spleen or tap a chest to hear fluid in the lungs. This emphasis on observation helped establish diagnostic reasoning as a defining skill of internists.
Carl von Rokitansky, Vienna’s pathology whiz, took medical investigation to a new level by performing over 60,000 autopsies. He connected what doctors saw in living patients with what he found under the microscope, like showing how pneumonia scarred a patient’s lungs, or heart failure caused fluid buildup. This clinicopathological correlation transformed diagnosis from guesswork into science, helping doctors better understand diseases like endocarditis, nephritis, liver cirrhosis, and pulmonary embolism. His meticulous findings and notes, detailing everything from swollen kidneys to inflamed heart valves, were a goldmine for internists. His work laid the groundwork for a deeper understanding of systemic diseases, from the slow creep of kidney failure to the sudden devastation of a pulmonary embolism.
By the mid-1800s, internists were the ultimate comprehensive physicians, treating the entire body as an interconnected system. Armed with little more than a stethoscope, thermometer, and physical examination, they laid the groundwork for modern medical diagnostics. This era wasn’t just the birth of a specialty. It was a revolution in how doctors tackled the body’s deepest mysteries, blending curiosity with a growing scientific rigor that set the stage for centuries of progress.
Growth and Institutionalization in the 19th and Early 20th Century
By the late 1800s, internal medicine was no longer a fledgling discipline but a well-established field with a clear place in the medical world.
Rudolf Virchow, often called the father of cellular pathology, was a German polymath who flipped medicine on its head by demonstrating that disease originates at the cellular level rather than from imbalanced “humors.” He’d spend hours peering through microscopes, spotting abnormal cells that explained why a patient’s blood wouldn’t clot or why their lungs failed. His discoveries explained previously misunderstood conditions such as leukemia, thrombosis, stroke, and inflammation, reshaping how internists understood disease progression. His work on thrombosis, for instance, helped internists understand why a patient might suddenly collapse from a pulmonary embolism, paving the way for better diagnosis and treatment.
Across the Atlantic, William Osler helped to define modern internal medicine. At Johns Hopkins Hospital, Osler emphasized bedside learning and holistic care. His textbook, The Principles and Practice of Medicine, became the internist’s bible, teaching physicians to integrate clinical observation, pathology, and compassion. Osler would spend hours noting a patient’s clammy skin, irregular pulse, or swollen ankles, teaching students to spot signs like the cherry-red spots of endocarditis or the clubbed fingers of lung disease. Osler’s enduring advice, “Listen to your patient; he is telling you the diagnosis,”remains central to internal medicine today.
This era saw internal medicine get organized, with major teaching hospitals like Johns Hopkins, Massachusetts General, and Berlin’s Charité becoming hubs of innovation where young doctors trained to think like internists.
Diagnostic tools got a major upgrade, too, supercharging practitioners’ clinical skills. The stethoscope, microscopy, and early laboratory tests enabled internists to detect heart murmurs, infections, anemia, and malignancy with unprecedented accuracy. By the early 20th century, internal medicine had become a structured, science-driven specialty grounded in patient care.
Mid-20th Century Advances: Laboratory and Technological Innovations
The mid-20th century marked a turning point for internal medicine, fueled by a tidal wave of scientific and technological breakthroughs. Laboratory testing expanded to include blood glucose, liver enzymes, and infection markers, while X-rays and electrocardiography (ECG) transformed diagnostic precision in the 1930s, allowing internists to peer inside the chest or abdomen, spotting pneumonia, heart enlargement, or early tumors without a scalpel. These innovative tools didn’t replace the bedside examination. They amplified it, making diagnoses faster, more precise, and more reliable. Across eras, internal medicine advances by integrating new data sources into clinical reasoning rather than replacing it.
The Rise of Subspecialties in Internal Medicine
This period also saw internal medicine branch out into a variety of subspecialties. Cardiology emerged to address heart attacks and arrhythmias, with internists mastering the art of interpreting ECGs to detect irregular rhythms. Endocrinology, focused on diabetes and thyroid disorders, equipped internists with tools to manage hormone imbalances. Gastroenterology addressed ulcers, hepatitis, and colon diseases, using new techniques such as barium studies to reveal gut blockages. Internists could now specialize, becoming experts in one organ system while staying rooted in the systemic thinking of internal medicine.
Still, the general internist remained essential, coordinating care across organ systems and managing patients with multiple chronic conditions. For example, recognizing how diabetes can systemically lead to kidney failure and heart disease in the same patient.
Perhaps the most transformative breakthrough was the introduction of antibiotics. Penicillin, mass-produced in the 1940s after Alexander Fleming’s 1928 discovery, turned deadly infections like bacterial endocarditis or sepsis into treatable conditions.
Combined with therapies such as insulin, corticosteroids to treat autoimmune diseases like lupus, and antihypertensive medications to address high blood pressure, internists had new tools to manage chronic conditions, solidifying internal medicine’s role at the heart of hospital and outpatient care.
Technologies like electrocardiography (ECG) enabled internists to map heart rhythms and spot atrial fibrillation and heart attacks in real time. Endoscopy and bronchoscopy opened windows into the gut and lungs, allowing internists to diagnose ulcers, tumors, or tuberculosis without invasive surgery.
By the 1960s, internal medicine was a powerhouse, with internists leading the charge in hospitals, clinics, and research labs, armed with tools that made them more effective than ever. This era cemented internal medicine as the brain trust of healthcare, blending science with the art of healing.
The Shift Toward Precision Medicine in Internal Medicine
Today, internal medicine is being reshaped by precision medicine, an approach that tailors treatment to a patient’s genetics, biomarkers, lifestyle, and environment. Genomic sequencing now allows internists to identify inherited risks for conditions such as heart disease, colorectal cancer, and Alzheimer’s disease. For internists, this means moving beyond generic treatment plans to individual care as unique as a patient’s DNA. Genomic sequencing now allows internists to identify inherited risks for conditions such as heart disease, colorectal cancer, and Alzheimer’s disease before symptoms appear.
For example, consider Lynch syndrome, a genetic mutation that skyrockets the risk of colon cancer. An internist might order earlier colonoscopies or preventive surgery, potentially saving a life. Biomarkers, measurable indicators like PSA for prostate cancer, troponins for heart attacks, or HbA1c for diabetes, give internists precise tools to diagnose and monitor. In diabetes care, continuous glucose monitors paired with genetic insights let internists fine-tune insulin regimens, keeping blood sugar steady and reducing complications such as nerve damage or blindness.
Targeted therapies are a hallmark of precision medicine. In oncology, drugs such as imatinib for chronic myeloid leukemia and pembrolizumab for lung cancer target specific genetic mutations. This spares healthy cells and boosts survival rates. Internists often coordinate these complex treatments, working with oncologists to manage side effects or monitor for complications.
Technology ties these advances together, with electronic health records integrating genetic data, lab results, and medical histories, and AI algorithms crunching data to predict risks such as heart attack or kidney failure before symptoms appear. This is precision medicine in action, making internal medicine more proactive and personalized, while also recognizing manageable challenges such as false positives, uncertain clinical significance, and the risk of overdiagnosis when data outpaces clear clinical pathways.
Current Trends and Future Directions
The next chapter of internal medicine will be shaped by growing medical complexity and expanding data, from genomics and biomarkers to wearables and AI-driven insights. Internists will increasingly translate these signals into clear diagnoses and coordinated care, while preserving human clinical judgment at the core of the specialty. To meet this moment, training programs and health systems must invest in education that integrates diagnostic reasoning, data science, population health, and team-based care. How effectively internal medicine balances innovation, equity, and clinical wisdom will determine its impact on patient outcomes in the years ahead.
Modern internal medicine already emphasizes team-based, coordinated care. Models such as Patient-Centered Medical Homes and Accountable Care Organizations position internists as care leaders, addressing both medical and social determinants of health. This collaborative approach ensures no detail is missed, particularly for patients navigating multiple chronic conditions.
Yet the expansion of precision medicine comes with hurdles. Genetic testing and targeted therapies can cost thousands of dollars, raising concerns about healthcare inequities and access. Data privacy remains a hot-button issue as genomic and health data become increasingly digitized and interconnected. Internists, already juggling packed schedules, must keep pace with a rapidly expanding body of research spanning genomics, AI, and population health. In response, training programs and professional organizations are evolving to equip internists for this changing landscape, while policy advocates push for more equitable access to precision care.
The future is nothing short of thrilling. Advances in AI, wearable technology, and gene-editing tools, such as CRISPR, hold promise for curing diseases like hemochromatosis, hypertrophic cardiomyopathy, and sickle cell anemia at their genetic roots. As healthcare shifts toward value-based care, internists will lead the charge, remaining essential in preventing disease, managing complexity, and delivering personalized treatment.
Precision, Compassion, Progress
From the candlelit origins of Innere Medizin to the high-tech era of precision medicine, internal medicine has continually evolved while preserving its core values: curiosity, rigor, and compassion. Guided by pioneers such as Schönlein, Virchow, and Osler, internists have shaped a specialty that blends science with humanity, while breakthroughs such as antibiotics, X-rays, and genomics have propelled the field into the history books. As medicine advances, internal medicine will remain the intellectual backbone of healthcare; adapting, innovating, and caring for patients as whole people.
Here’s to a future where every diagnosis is spot-on, every treatment is tailored, and every internist is a hero in a white coat, ready to tackle the next big challenge with a smile and a stethoscope.
Key Takeaways
- Internal medicine began with keen observation and diagnostic reasoning.
- Pioneers like Osler and Virchow transformed medical science and practice.
- Technological advances like X-rays and lab tests boosted diagnostic accuracy.
- Precision medicine tailors care using genetics, biomarkers, and AI.
- Internists remain central in coordinating complex, patient-focused care.
References
- https://www.ejinme.com/article/S0953-6205(07)00271-3/fulltext
- https://www.britannica.com/biography/Johann-Lukas-Schonlein
- https://www.britannica.com/biography/Karl-Freiherr-von-Rokitansky
- https://www.britannica.com/biography/Rudolf-Virchow
- https://www.britannica.com/biography/Sir-William-Osler-Baronet
- https://archive.org/details/principlesandpr00mccrgoog
- https://www.bmj.com/content/376/bmj.o646
- https://www.britannica.com/biography/Rene-Laennec
- https://www.osmosis.org/notes/Cardiovascular_Anatomy_and_Physiology
- https://www.osmosis.org/notes/Anatomy_and_Physiology_of_the_Endocrine_System
- https://www.osmosis.org/notes/Anatomy_and_Physiology_of_the_Gastrointestinal_System
- https://www.osmosis.org/learn/Diabetes_mellitus
- https://www.britannica.com/biography/Alexander-Fleming
- https://www.osmosis.org/learn/Autoimmunity:_Nursing
- https://www.osmosis.org/learn/ECG_basics
- https://research.ucalgary.ca/precision-medicine
- https://www.nih.gov/about-nih/nih-turning-discovery-into-health/promise-precision-medicine
- https://www.osmosis.org/learn/Genomics_-_Ethical%2C_legal%2C_and_social_implications_(ELSI)%3A_Nursing
- https://www.mayoclinic.org/diseases-conditions/lynch-syndrome/symptoms-causes/syc-20374714
- https://pmc.ncbi.nlm.nih.gov/articles/PMC5813875/
- https://www.cancer.gov/about-cancer/treatment/types/targeted-therapies
- https://pmc.ncbi.nlm.nih.gov/articles/PMC9374078/
- https://www.cms.gov/priorities/innovation/key-concepts/accountable-care-and-accountable-care-organizations
- https://www.ncqa.org/programs/health-care-providers-practices/patient-centered-medical-home-pcmh/
- https://news.stanford.edu/stories/2024/06/stanford-explainer-crispr-gene-editing-and-beyond
- https://kevinmd.com/2019/10/how-internal-medicine-got-its-name.html
- https://www.acponline.org/about-acp/about-internal-medicine/career-paths/medical-student-career-path/history-of-internal-medicine
- https://www.acpjournals.org/doi/10.7326/0003-4819-105-3-452_1
- https://pubmed.ncbi.nlm.nih.gov/2651599/
- https://pmc.ncbi.nlm.nih.gov/articles/PMC1494912/
- https://www.amjmed.com/article/S0002-9343(05)01038-7/fulltext
- https://www.adventhealth.com/primary-care-plus/blog/internal-medicine-vs-primary-care-comparison-guide
- https://www.ejinme.com/article/S0953-6205(21)00430-1/fulltext
- https://www.mdpi.com/2075-4426/14/4/418

Try Osmosis from Elsevier today! Access your free trial and discover why millions of current and future clinicians and caregivers love learning by Osmosis.
Leave a Reply