
This week, we are sharing another USMLE® Step 1-style practice question to test your knowledge of medical topics. Today’s case focuses on a 72-year-old man with fatigue and progressive dyspnea. Physical examination shows 3+ edema in the lower extremities and hepatomegaly. Can you figure it out?
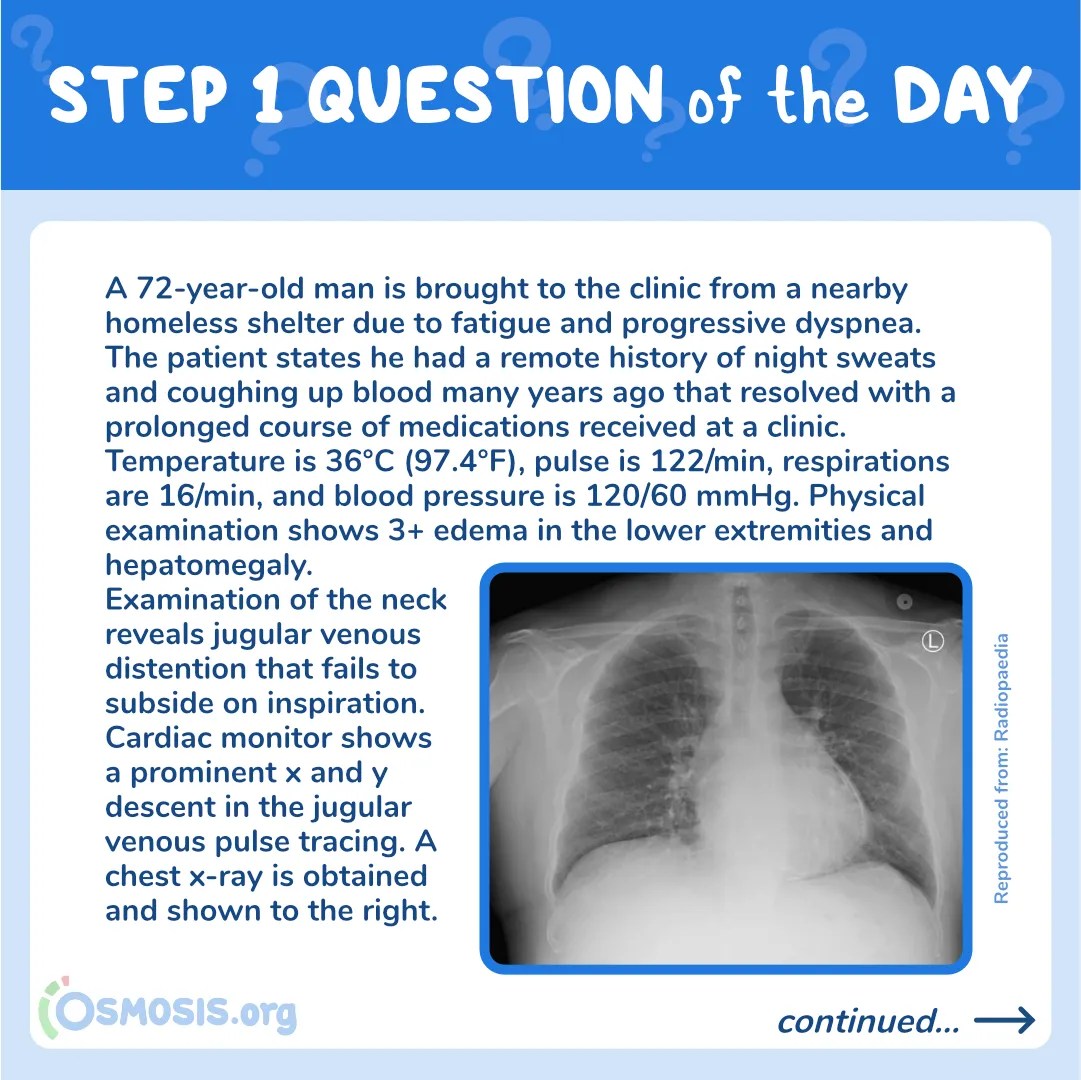
A 72-year-old man is brought to the clinic from a nearby homeless shelter due to fatigue and progressive dyspnea. The patient states he had a remote history of night sweats and coughing up blood many years ago that resolved with a prolonged course of medications received at a clinic. Temperature is 36°C (97.4°F), pulse is 122/min, respirations are 16/min, and blood pressure is 120/60 mmHg. Physical examination shows 3+ edema in the lower extremities and hepatomegaly. Examination of the neck reveals jugular venous distention that fails to subside on inspiration. Cardiac monitor shows a prominent x and y descent in the jugular venous pulse tracing. A chest x-ray is obtained and shown below:

Reproduced from: Radiopaedia
Which of the following is the most likely cause of this patient’s condition?
A. Cardiac myxoma
B. Constrictive pericarditis
C. Dilated cardiomyopathy
D. Hypertrophic obstructive cardiomyopathy
E. Restrictive cardiomyopathy
Scroll down to find the answer!
The correct answer to today’s USMLE® Step 1 Question is…
B. Constrictive pericarditis
Before we get to the Main Explanation, let’s look at the incorrect answer explanations. Skip to the bottom if you want to see the correct answer right away!
Incorrect answer explanations
The incorrect answers to today’s USMLE® Step 1 Question are…
A. Cardiac myxoma
Incorrect: Cardiac myxoma is the most common cardiac tumor in adults. Myxomas are typically described as a “ball-valve” mass found in the left atrium. Patients often present with fever, weight loss, and possible syncopal episodes. Cardiac auscultation may reveal an early diastolic “tumor plop” sound. Cardiac myxoma, however, does not cause calcifications of the myocardium or jugular venous pulse changes, as seen in this patient.
C. Dilated cardiomyopathy
Incorrect: Dilated cardiomyopathy can also present with dyspnea, chest pain, and edema. Causes of dilated cardiomyopathy include genetics, substance abuse (e.g., alcohol, cocaine), and certain infections. Dilated cardiomyopathy, however, does not cause calcifications of the myocardium or jugular venous pulse changes, as seen in this patient.
D. Hypertrophic obstructive cardiomyopathy
Incorrect: Hypertrophic obstructive cardiomyopathy is the most common cause of death in young athletes. It is caused by hypertrophy of the myocardium. Patients often present with a harsh systolic ejection murmur and a palpable apical impulse, neither of which are seen in this patient.
E. Restrictive cardiomyopathy
Incorrect: The presentation of restrictive cardiomyopathy is very similar to constrictive pericarditis, including chest pain, dyspnea, edema, fatigue, and exercise intolerance due to elevations in filling pressures. The history and physical examination may differentiate the cause. Causes of restrictive cardiomyopathy include post-radiation fibrosis, Löffler endocarditis, amyloidosis, sarcoidosis, and hemochromatosis. In contrast to constrictive pericarditis, restrictive cardiomyopathy presents with prominent y descent but blunting of the x descent in the jugular venous pulse. Additionally, an echocardiogram may reveal an increase in wall thickness rather than the calcifications on the chest radiograph seen in this patient.

Main Explanation
This patient’s presentation is consistent with constrictive pericarditis, a condition characterized by incomplete filling of the cardiac chambers due to thickening of the pericardium (seen as a line of calcifications over the heart border on the chest radiograph). This patient experiencing homelessness likely had a previous history of tuberculosis infection (hemoptysis, night sweats), a common cause of constrictive pericarditis. Other causes of constrictive cardiomyopathy include post-cardiac surgery or radiation, connective tissue disorder, and miscellaneous causes (e.g., malignancy, trauma, drug-induced sarcoidosis, uremic pericarditis). Note that some of the causes are common to both restrictive cardiomyopathy and constrictive pericarditis.
The fibrous thickening of the pericardium forms a rigid, noncompliant cover of the heart, resulting in progressive impairment in cardiac filling with subsequent low cardiac output. The impaired heart filling leads to progressive signs and symptoms of predominantly right heart failure (e.g., pitting edema of the lower extremities and hepatomegaly). Patients often present with fluid overload, ranging from peripheral edema to anasarca, and symptoms related to low cardiac output, such as fatigue and dyspnea on exertion. On physical examination, the majority of patients display elevated jugular venous pressure. Other less common features include pulsus paradoxus, Kussmaul sign (increase or lack of decrease in JVP during inspiration), pericardial knock, peripheral edema, ascites, and/or cachexia. Pericardial knock is a unique feature that can be heard during early diastole. The sound corresponds to the abrupt cessation of ventricular filling due to a constrictive pericardium. Jugular venous pulse tracing typically reveals prominent x and y descent, correlating with the downward displacement of closed tricuspid valves during rapid ventricular ejection and right atrial emptying, respectively.
The diagnosis of constrictive pericarditis is commonly made using echocardiography in patients presenting with high clinical suspicion. Depending on the severity, patients may be treated with medications aimed at reducing inflammation (colchicine and NSAIDs) or pericardiectomy surgery.
Major Takeaway
Constrictive pericarditis is a condition characterized by impaired filling of the heart due to thickening of the pericardium. Patients often present with signs of right heart failure, including fatigue, edema, hepatomegaly, and dyspnea. On imaging, calcifications and thickening of the pericardium may be seen.
References
Geske, J. B., Anavekar, N. S., Nishimura, R. A., Oh, J. K., & Gersh, B. J. (2016, November 21). Differentiation of Constriction and Restriction: Complex Cardiovascular Hemodynamics.
Welch, T. D., & Oh, J. K. (2017). Constrictive Pericarditis. Cardiology Clinics, 35(4), 539–549. doi:10.1016/j.ccl.2017.07.007
_________________________
Want more USMLE® Step 1 practice questions? Try Osmosis today! Access your free trial and find out why millions of current and future clinicians and caregivers love learning with us.

Leave a Reply