
Discover the case of a 42-year-old man with knee pain, red eyes, and foot lesions post-UTI treatment. Could it be reactive arthritis?
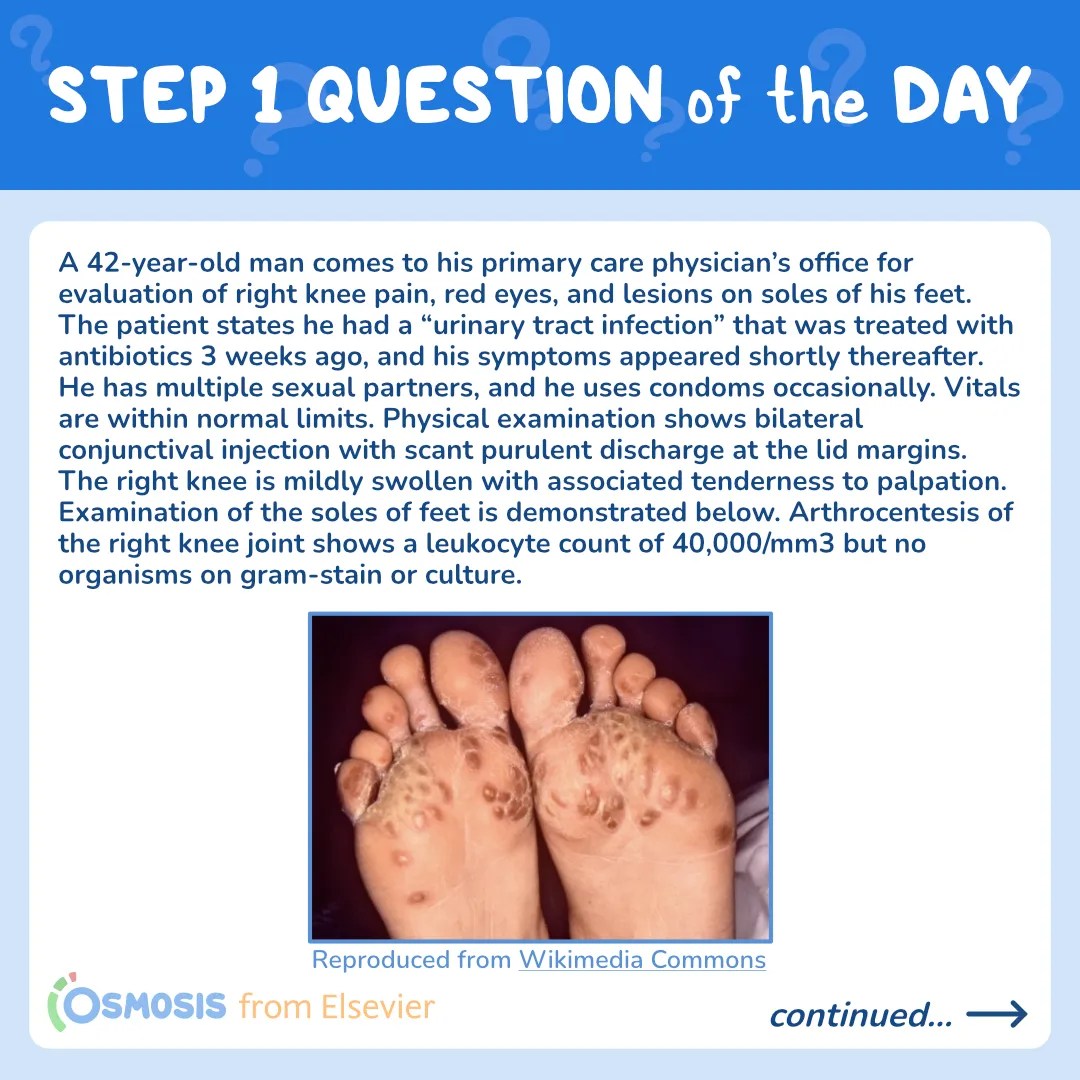
A 42-year-old man comes to his primary care physician’s office for evaluation of right knee pain, red eyes, and lesions on soles of his feet. The patient states he had a “urinary tract infection” that was treated with antibiotics 3 weeks ago, and his symptoms appeared shortly thereafter. He has multiple sexual partners, and he uses condoms occasionally. Vitals are within normal limits. Physical examination shows bilateral conjunctival injection with scant purulent discharge at the lid margins. The right knee is mildly swollen with associated tenderness to palpation. Examination of the soles of feet is demonstrated below. Arthrocentesis of the right knee joint shows a leukocyte count of 40,000/mm3 but no organisms on gram-stain or culture. Which of the following is the most likely diagnosis?

Retrieved from: Wikimedia Commons
A. Ankylosing spondylitis
B. Reactive arthritis
C. Psoriatic arthritis
D. Septic arthritis
E. Gout
Scroll down for the correct answer!
The correct answer to today’s USMLE® Step 1 Question is…
B. Reactive arthritis
Before we get to the Main Explanation, let’s look at the incorrect answer explanations. Skip to the bottom if you want to see the correct answer right away!
Incorrect answer explanations
A. Ankylosing spondylitis
Incorrect: Ankylosing spondylitis is a chronic inflammatory condition that presents with low back pain and morning stiffness. Although it is also a seronegative arthropathy, it is not associated with a recent infectious process.
C. Psoriatic arthritis
Incorrect:Psoriatic arthritis is another seronegative arthropathy that occurs in conjunction with psoriatic skin lesions, which are well-defined scaly erythematous plaques on extensor surfaces. An antecedent urinary tract infection and hyperkeratotic vesicles on palms and soles are atypical.
D. Septic arthritis
Incorrect: Septic arthritis usually results from inoculation of Staph aureus and presents with fever and severe, focal joint pain. Examination typically shows an erythematous tender swollen joint with associated effusion. Arthrocentesis normally reveals synovial fluid leukocytes >50,000/mm3 and gram positive organisms on gram stain as well as culture.
E. Gout
Incorrect: Gout typically presents with acute onset (<12 hours) pain and swelling in the affected joint–usually the great toe. Synovial fluid analysis reveals negatively birefringent needle-shaped crystals. Vesicular lesions and conjunctivitis are not associated with gout.
Main Explanation

This patient presents with right knee pain and swelling, bilateral conjunctivitis and a history suspicious for chlamydial urethritis, consistent with reactive arthritis (formerly called Reiter syndrome). The erythematous scaly lesions on the soles are keratoderma blennorrhagica, the cutaneous manifestation of reactive arthritis.
Reactive arthritis occurs days to weeks following a urinary tract or gastrointestinal tract infection, and it is thought to be an autoimmune process triggered by molecular mimicry, rather than a pathogen directly infecting the joint. It is highly associated with HLA-B27 haplotype. Causative organisms include Chlamydia, Yersinia, Salmonella, Shigella, and Campylobacter. It usually presents with a triad of asymmetric oligoarthritis (especially involving knee joint), conjunctivitis and urethritis. Other features include enthesitis (inflammation at the tendon or ligament insertion site), dactylitis (sausage digits) and sacroiliitis. Common extra-articular manifestations include oral ulcers, keratoderma blennorrhagica (as in this patient) and circinate balanitis (painless erythematous lesions with small, shallow ulcers on the glans penis).
Major Takeaway
Reactive arthritis is an HLA-B27-associated arthropathy that usually presents with a triad of urethritis, conjunctivitis and oligoarticular sterile arthritis. It generally follows a genitourinary or enteric infection. Extra-articular manifestations include oral ulcers, keratoderma blennorrhagica and circinate balanitis.
References
- Hannu, T. (2011). Reactive arthritis. Best Practice & Research Clinical Rheumatology, 25(3), 347-357.
- Carter, J. D., & Hudson, A. P. (2009). Reactive arthritis: clinical aspects and medical management. Rheumatic Disease Clinics, 35(1), 21-44.
________________________
Want more USMLE® Step 1 practice questions? Try Osmosis by Elsevier today! Access your free trial and find out why millions of current and future clinicians and caregivers love learning with us.

The United States Medical Licensing Examination (USMLE®) is a joint program of the Federation of State Medical Boards (FSMB®) and National Board of Medical Examiners (NBME®). Osmosis is not affiliated with NBME nor FSMB.
Leave a Reply