
Each week, Osmosis shares a USMLE® Step 1-style practice question to test your knowledge of medical topics. Today’s case involves a 4-year-old boy with progressive lethargy, headaches, and worsening vision. A brain MRI shows a lesion in the fourth ventricle with dilated ventricles. Can you figure the most likely diagnosis?
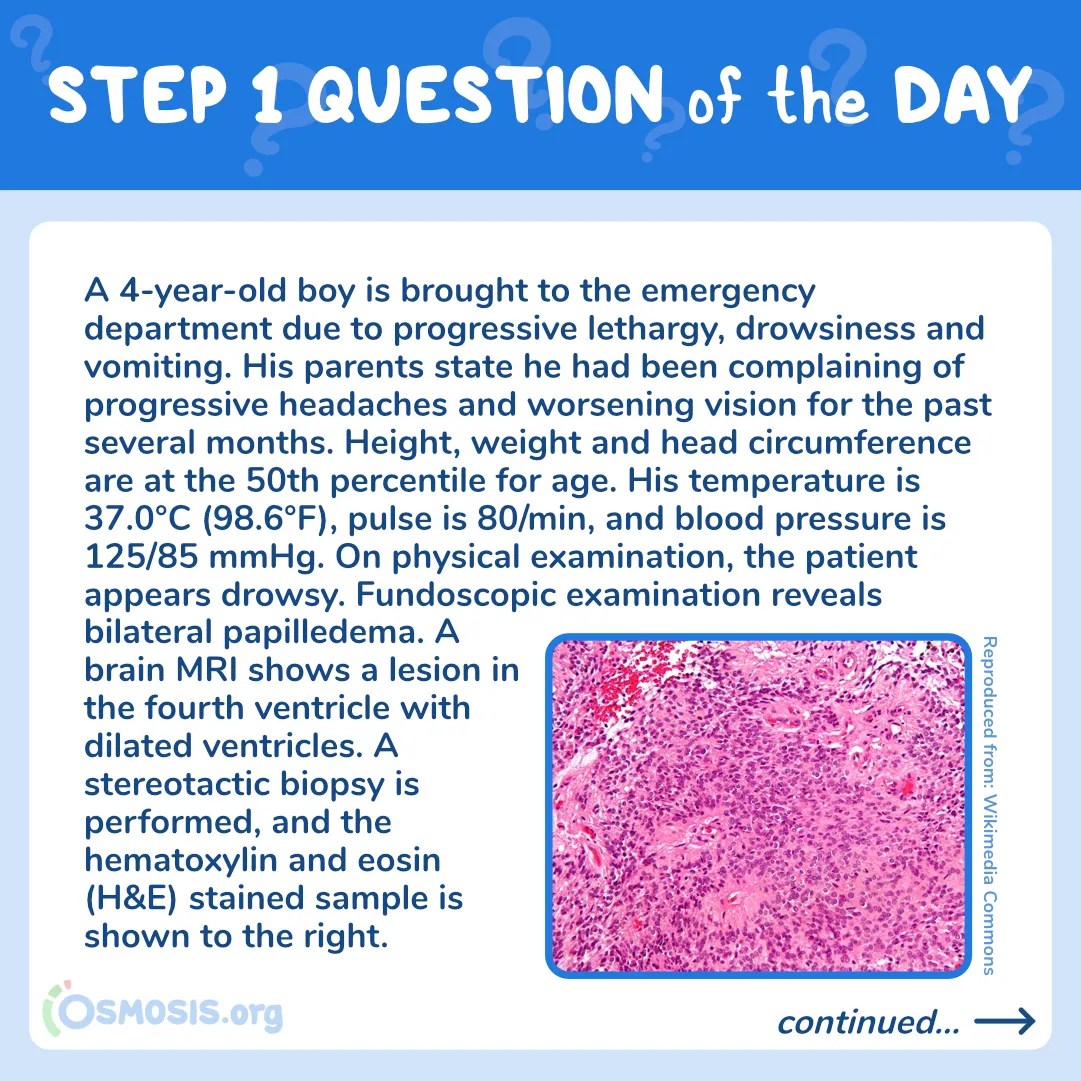
A 4-year-old boy is brought to the emergency department due to progressive lethargy, drowsiness and vomiting. His parents state he had been complaining of progressive headaches and worsening vision for the past several months. Height, weight and head circumference are at the 50th percentile for age. His temperature is 37.0°C (98.6°F), pulse is 80/min, and blood pressure is 125/85 mmHg. On physical examination, the patient appears drowsy. Fundoscopic examination reveals bilateral papilledema. A brain MRI shows a lesion in the fourth ventricle with dilated ventricles. A stereotactic biopsy is performed, and the hematoxylin and eosin (H&E) stained sample is shown below.

Reproduced from: Wikimedia CommonsWhat is the most likely diagnosis in this patient?
A. Craniopharyngioma
B. Ependymoma
C. Medulloblastoma
D. Pilocytic astrocytoma
E. OligodendrogliomaScroll down to find the answer!
→ Reinforce your understanding with more self-assessment items on Osmosis.
The correct answer to today’s USMLE® Step 1 Question is…
B. Ependymoma
Before we get to the Main Explanation, let’s look at the incorrect answer explanations. Skip to the bottom if you want to see the correct answer right away!
Incorrect answer explanations
The incorrect answers to today’s USMLE® Step 1 Question are…
A. Craniopharyngioma
Incorrect: Craniopharyngiomas, while common, would be located in the pituitary fossa. Patients may present with bitemporal hemianopsia due to compression of the optic chiasm. Calcifications are often seen on imaging. On light microscopy, keratin pearls and cysts filled with cholesterol crystals (“motor oil”-like) are expected. The location and histology findings of this patient’s tumor favors another diagnosis.
C. Medulloblastoma
Incorrect: Medulloblastomas are poorly-differentiated, highly-malignant tumors seen exclusively in children. These tumors commonly arise from the cerebellum and are characterized by Homer-Wright rosettes on histology. Common symptoms are ataxia, slurred speech, nystagmus, positive Romberg sign, and intention tremor. This patient’s imaging and histological findings favor another diagnosis.
D. Pilocytic astrocytoma
Incorrect: Pilocytic astrocytoma, the most common pediatric primary brain tumor, is a benign low-grade tumor that usually arises in the cerebellar hemispheres or around the third ventricle. On imaging, cystic and solid components can be seen. Under light microscopy, it stains positive for glial fibrillary acidic protein (GFAP) and shows eosinophilic corkscrew fibers (Rosenthal fibers). The location and histology findings of this patient’s tumor favors another diagnosis.
E. Oligodendroglioma
Incorrect: Oligodendrogliomas are malignant tumors that generally occur in adults. They are rare tumors of oligodendrocyte origin that often grow in the frontal lobes. On histology, cells have round nuclei with clear cytoplasm forming a “fried egg” appearance and the capillaries of the tumor are arranged in a “chicken-wire” pattern. Calcifications may also be seen on imaging. The location, patient age, and histology findings favor another diagnosis.

Main Explanation
The progressive symptoms of hydrocephalus (lethargy, nausea, vomiting), the location of the tumor (4th ventricle), and the characteristic perivascular pseudorosettes in the biopsy specimen all point to an ependymoma.
Ependymomas are invasive primary brain tumors that arise from the glial cells lining the ventricular system. Most commonly they occur in the 4th ventricle, leading to hydrocephalus. Ependymomas have the potential to disseminate throughout the central nervous system (CNS). Similar to medulloblastoma, the tumor can send metastasis to the spinal cord; however, on histology, the tumor is distinguished by perivascular pseudorosettes, not Homer-Wright rosettes (as seen in medulloblastoma). Pseudorosettes are neoplastic cells arranged around a blood vessel, while Homer-Wright rosettes are instead arrangements of small blue cells around a central core.
Resection and adjuvant radiation therapy are the mainstays of treatment, except in very young patients. Chemotherapy is used only in very young children, patients with bulky residual disease, and recurrent or refractory tumors.

Major Takeaway
Ependymomas are invasive brain tumors that arise from the glial cells lining the ventricular system. Most commonly they occur in the 4th ventricle, leading to hydrocephalus. On histology, cells form characteristic perivascular pseudorosettes.
References
Shuangshoti S, Rushing EJ, Mena H, Olsen C, Sandberg GD. Supratentorial extraventricular ependymal neoplasms: a clinicopathologic study of 32 patients. Cancer. 2005;103(12):2598-2605. doi:10.1002/cncr.21111
_________________________
Want more USMLE® Step 1 practice questions? Try Osmosis today! Access your free trial and find out why millions of current and future clinicians and caregivers love learning with us.

The United States Medical Licensing Examination (USMLE®) is a joint program of the Federation of State Medical Boards (FSMB®) and National Board of Medical Examiners (NBME®). Osmosis is not affiliated with NBME nor FSMB.
Leave a Reply