
This week, we are sharing another USMLE® Step 1-style practice question to test your knowledge of medical topics. Today’s case involves a 65-year-old man who suddenly collapsed when crossing the street. An electrocardiogram is demonstrated below. Can you figure out which pathophysiologic process is likely the result of this cardiac activity?
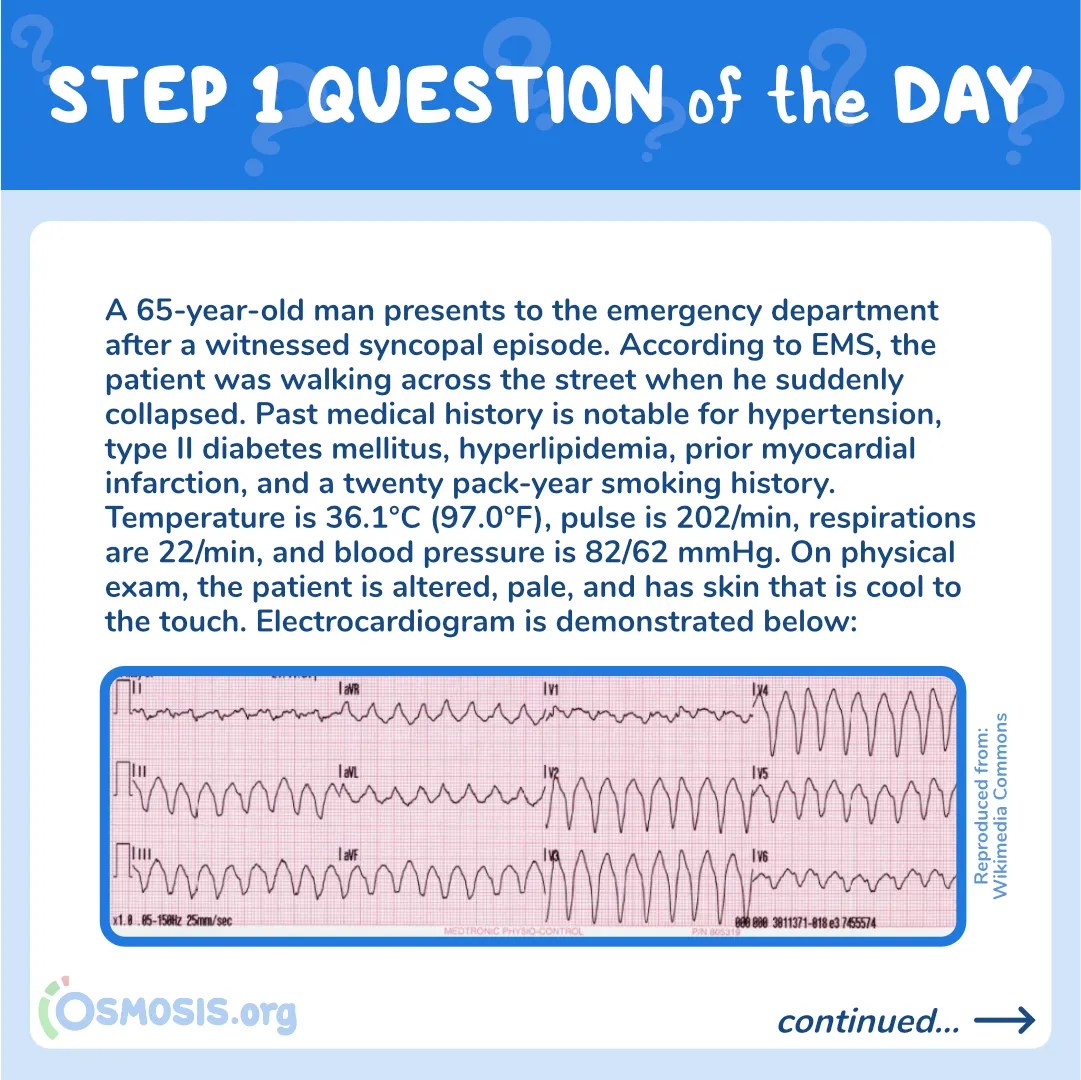
A 65-year-old man presents to the emergency department after a witnessed syncopal episode. According to EMS, the patient was walking across the street when he suddenly collapsed. Past medical history is notable for hypertension, type II diabetes mellitus, hyperlipidemia, prior myocardial infarction, and a twenty pack-year smoking history. Temperature is 36.1°C (97.0°F), pulse is 202/min, respirations are 22/min, and blood pressure is 82/62 mmHg. On physical exam, the patient is altered, pale, and has skin that is cool to the touch. Electrocardiogram is demonstrated below:

Image reproduced from Wikimedia Commons
Based on this patient’s clinical presentation, this cardiac activity is likely the result of which of the following pathophysiologic processes?
A. Re-entrant conduction below or within the bundle of His
B. Aberrant conduction through the bundle of Kent
C. Enhanced automaticity from the tricuspid annulus
D. Multiple atrial micro-reentrant circuits
E. Reentry circuit within the AV node
Scroll down to find the answer!
→ Reinforce your understanding with more self-assessment items on Osmosis
The correct answer to today’s USMLE® Step 1 Question is…
A. Re-entrant conduction below or within the bundle of His
Before we get to the Main Explanation, let’s look at the incorrect answer explanations. Skip to the bottom if you want to see the correct answer right away!
Incorrect answer explanations
The incorrect answers to today’s USMLE® Step 1 Question are…
B. Aberrant conduction through the bundle of Kent
Incorrect: Pre-excitation syndromes such as Wolff-Parkinson White (WPW) are characterized by an accessory bypass tract. WPW is electrocardiographically characterized by a delta wave, broad QRS complexes, and short PR interval.
C. Enhanced automaticity from the tricuspid annulus
Incorrect: Multifocal atrial tachycardia (MAT) is defined by an irregularly irregular rhythm with varying intervals and at least 3 distinct P-wave morphologies in the same lead. Patients with underlying pulmonary disease are predisposed to this tachyarrhythmia; however, this patient’s rhythm is regular, and the QRS complexes are wide.
D. Multiple atrial micro-reentrant circuits
Incorrect: Atrial fibrillation is defined electrocardiographically as irregularly irregular QRS complexes with absent p-waves; the impulse originates from multiple atrial micro-reentrant circuits. This patient’s rhythm is regular, and the QRS complexes are wide.
E. Reentry circuit within the AV node
Incorrect: Paroxysmal supraventricular tachycardia presents with a heart rate ranging between 150 to 250 beats per minute, a narrow QRS complex, and in some cases, absent p-waves. This patient’s electrocardiogram demonstrates wide QRS complexes.

Main Explanation
This patient presents after a witnessed syncopal episode with unstable vital signs and electrocardiogram demonstrating monomorphic ventricular tachycardia in the setting of a history of coronary artery disease. Of the answer choices listed, the most likely etiology of this patient’s arrhythmia is an aberrant re-entry mechanism at or below the bundle of His.
Ventricular tachycardia refers to an ectopic focus of electrical activity within the ventricle. The condition is electrocardiographically characterized by a rapid heart rate (>100 beats per minute) and wide QRS complexes (>120 ms). In general, ventricular tachycardia is further subdivided into monomorphic and polymorphic forms.
Monomorphic ventricular tachycardia presents with QRS complexes that have a uniform appearance–meaning all of the QRS complexes are identical. Monomorphic ventricular tachycardia is classically associated with myocardial scarring, acute myocardial infarction, or structural heart disease. Polymorphic ventricular tachycardia is characterized by multiple ventricular foci and resultant QRS complexes that vary in amplitude, axis, and duration. Polymorphic ventricular tachycardia can be associated with cardiac ischemia, although it is more commonly due to underlying metabolic derangements, medication toxicities, or inherited channelopathies (e.g., Brugada syndrome, Romano-Ward syndrome).
Major Takeaway
Ventricular tachycardia refers to an ectopic focus of electrical activity within the ventricle that is electrocardiographically characterized by a rapid heart rate (>100 beats per minute) and wide QRS complexes (>120 ms). It is most commonly due to a reentry mechanism at or within the bundle His.
References
Jameson, J.L. (2018) Harrison’s principles of internal medicine. New York: McGraw-Hill Education. ISBN: 9781259644030.
Kumar, V., Abbas, A.K., Aster, J.C., Perkins, J.A., Robbins, S.L. (2018) Robbins basic pathology (10th ed.). Philadelphia, PA: Elsevier. ISBN: 978-0-323-35317-5.
Walls, R., Hockberger, R., Gausche-Hill, M. (2017) Rosen’s Emergency Medicine: Concepts and Clinical Practice. Philadelphia, PA: Elsevier. ISBN: 978-0323354790.
_________________________
Want more USMLE® Step 1 practice questions? Try Osmosis today! Access your free trial and find out why millions of current and future clinicians and caregivers love learning with us.

The United States Medical Licensing Examination (USMLE®) is a joint program of the Federation of State Medical Boards (FSMB®) and National Board of Medical Examiners (NBME®). Osmosis is not affiliated with NBME nor FSMB.
Leave a Reply