
Today, we’re examining a clinical case of a 4-year-old child in the ER with elbow pain. What’s the the likely cause?
A 4-year-old boy is brought to the emergency department by his mother to be evaluated for elbow pain. He was forcefully pulled onto the curb by his mother after inadvertently stepping into the street. The patient has refused to move his right arm since the incident. Vitals are within normal limits. Physical examination shows an irritable child holding his right upper limb with his left hand. The affected elbow is flexed and the forearm pronated. There is no visible erythema, swelling, or deformity. There is limited range of motion on physical examination.
Which of the following structures is most likely involved in this patient’s condition?
A. Biceps tendon
B. Annular ligament
C. Lateral epicondyle tendon
D. Medial epicondyle tendon
E. Interosseous membrane of the forearm
Scroll down for the correct answer!
The correct answer to today’s USMLE® Step 2 Question is…
B. Annular ligament
Correct: See Main Explanation.
Incorrect Answer Explanations
A. Biceps tendon
Incorrect: Biceps tendon rupture typically occurs in older adults secondary to forceful extension of the elbow on a fully contracted biceps muscle. Patients may hear or feel a “popping” sensation. There is often a visible ‘Popeye deformity’ in the mid-upper arm reflective of the shortened biceps brachii. Limited range of motion at the elbow joint as seen in this patient would not be expected.
C. Lateral epicondyle tendon
Incorrect: Lateral epicondyle tendonitis can cause pain and tenderness at the lateral elbow. However with this condition there is full range of motion of the elbow joint.
D. Medial epicondyle tendon
Incorrect: Medial epicondyle tendonitis can cause pain and tenderness at the medial epicondyle. However with this condition there is full range of motion of the elbow joint.
E. Interosseous membrane of the forearm
Incorrect: The interosseous membrane of the forearm is a connective tissue that lies between the radius and ulna. It is usually affected in patients with a radius or ulna fractures following a fall on an outstretched hand.
Main Explanation
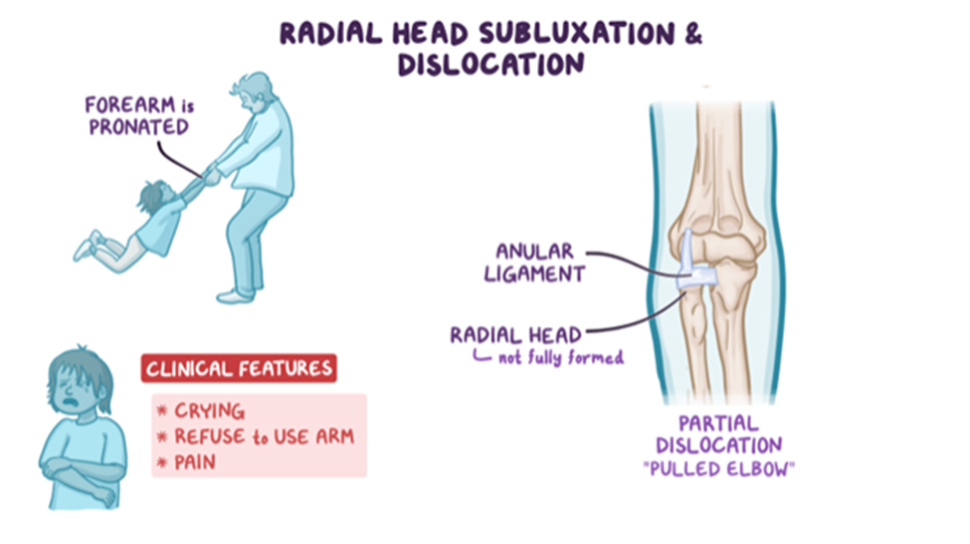
Radial head subluxation (i.e. nursemaid’s elbow) is a common injury in young children (1-4 years of age). It is the most common upper extremity injury in infants and young children presenting to the emergency department. It is typically caused by axial traction on an outstretched, pronated forearm. With sudden traction on the distal radius, the annular ligament slips over the head of the radius at the level of the radiohumeral joint, where it becomes entrapped.
Children with radial head subluxationIt typically present holding the injured arm in a flexed and pronated position and refusing to move it. Patients present with sudden, acute pain of the affected arm. Notably, pain does not always localize to the elbow and there is typically no swelling, bruising, or deformity of the arm. The diagnosis is clinical and most patients can be managed with closed manual reduction by either hyperpronation of the forearm (preferred) or supination of the forearm with flexion of the elbow.
Major Takeaway
Radial head subluxation (i.e. nursemaid’s elbow) refers to a displacement of the annular ligament over the head of the radius and entrapment of the annular ligament in the radiohumeral joint. It results from axial traction on an outstretched pronated forearm, typically in a child <5 years of age.
Want to learn more about this topic?
Watch the Osmosis video: Anterior cruciate ligament injury
References
- Welch, R., Chounthirath, T., & Smith, G. A. (2017). Radial head subluxation among young children in the United States associated with consumer products and recreational activities. Clinical Pediatrics, 56(8), 707-715.
- Rudloe, T. F., Schutzman, S., Lee, L. K., & Kimia, A. A. (2012). No longer a “nursemaid’s” elbow: mechanisms, caregivers, and prevention. Pediatric emergency care, 28(8), 771-774.
- Hill, C. E., & Cooke, S. (2017). Suppl-8, M6: Common Paediatric Elbow Injuries. The open orthopaedics journal, 11, 1380.
- Boutis K (2020). Pediatric orthopedic emergencies. Tintinalli J.E., & Ma O, & Yealy D.M., & Meckler G.D., & Stapczynski J, & Cline D.M., & Thomas S.H.(Eds.), Tintinalli’s Emergency Medicine: A Comprehensive Study Guide, 9e. McGraw-Hill.

Want more USMLE® Step 2 CK practice questions? Try Osmosis by Elsevier today! Access your free trial and discover why millions of current and future clinicians and caregivers love learning with us.
Leave a Reply