
A child arrives in the ED after a sledding accident causes some head trauma. What are the next steps in the child’s care? Do you know? Let’s find out!
A 9-year-old boy is brought to the emergency department by his parent for evaluation of a closed head injury. He was on a sled traveling downhill when he collided with a tree striking his forehead on the ground. He was not wearing a helmet and lost consciousness for about 30 seconds. The patient has no significant past medical history and takes no medication. Temperature is 37.5°C (99.5°F), pulse is 110/min, respirations are 22/min, blood pressure is 100/75 mmHg, and oxygen saturation is 99% on room air. Upon arrival, a cervical collar is placed. The patient is speaking in clear full sentences but appears confused. There is a large hematoma over the forehead. The patient is moving all extremities spontaneously and localizes to pain and opens his eyes spontaneously. A full head-to-toe examination does not reveal any further injury or trauma.
Which of the following is the best next step in management?
A. Intubate the patient
B. Administer mannitol
C. Elevate the head of the bed
D. Calculate Glasgow coma scale
E. Obtain magnetic resonance imaging (MRI) of the brain
Scroll down for the correct answer!
The correct answer to today’s USMLE® Step 2 Question is…
D. Calculate Glasgow coma scale
Correct: See Main Explanation.
Incorrect Answer Explanations
A. Intubate the patient
Incorrect: This patient, while confused, is currently protecting his airway and therefore does not need intubation. He should have a Glasgow Coma Scale (GCS) calculated before proceeding with further management.
B. Administer mannitol
Incorrect: This patient does not have documented radiographic findings of intracranial hemorrhage warranting the administration of mannitol.
C. Elevate the head of the bed
Incorrect: The head of the bed should be elevated to at least 30 degrees for patients with documented evidence of intracranial hemorrhage. This patient does not have documented radiographic findings of intracranial hemorrhage.
E. Obtain magnetic resonance imaging (MRI) of the brain
Incorrect: A plain head computed tomography (CT) is typically pursued over MRI for pediatric head trauma patients due to the time-sensitive nature of possible life-threatening diagnoses; however, this patient should first have a Glasgow Coma Scale (GCS) calculated.
Main Explanation

This 9-year-old boy presents to the emergency department for evaluation of a traumatic brain injury (TBI) following a sledding accident. A critical component of acute management for pediatric patients with TBI is to calculate a Glasgow Coma Scale (GCS). This score’s results guide further management, including the need for advanced imaging or airway support (e.g. intubation).
TBI refers to brain damage that results from an external mechanism, like a fall, motor vehicle accident, or non-accidental trauma. When a pediatric patient presents with a TBI, it is important to stabilize them urgently, assess the severity of the injury, and determine the need for imaging.
Primary survey should be performed by assessing the airway, breathing, and circulation; and immobilization of the neck and spine should be performed. Additional supportive measures should include obtaining intravenous (IV) access, starting IV fluids, continuously monitoring vital signs, and providing supplemental oxygen if needed. Next, a Glasgow Coma Scale, or GCS should be calculated.
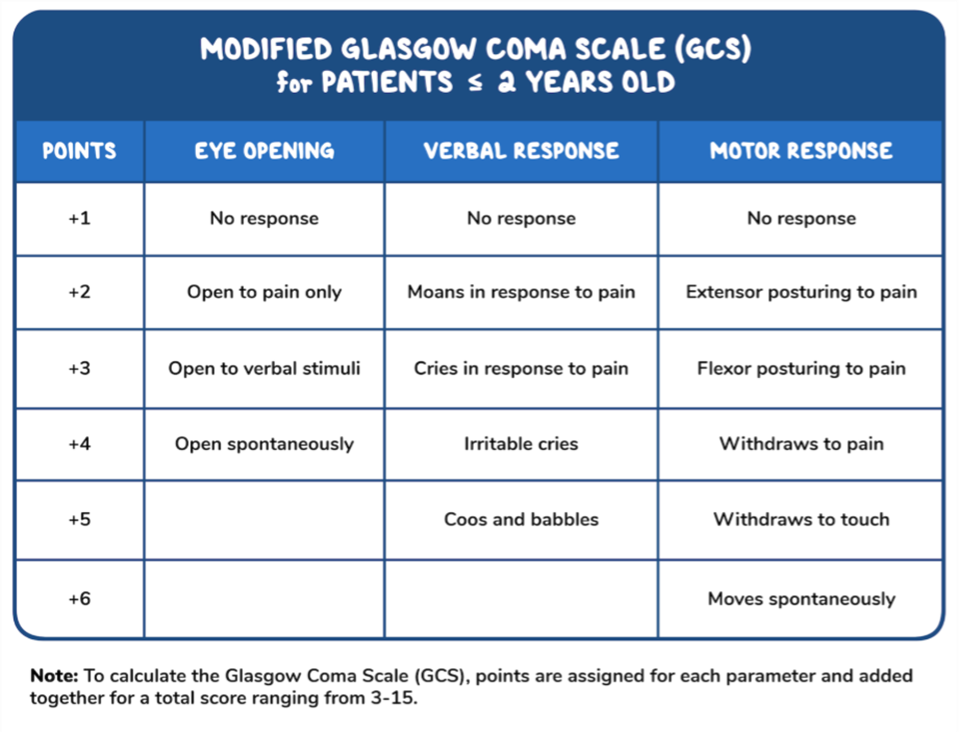
This scale assesses the patient’s eye opening in addition to their motor and verbal responses, to determine their level of consciousness and need for imaging or additional airway support. In general, patients with a GCS of less than 8 should be considered for intubation (a helpful rhyme is “GCS of eight means you intubate!”). In addition, the GCS provides an objective measurement to assess the degree of brain injury. For children under two years of age, a modified Pediatric GCS can be used instead.
Major Takeaway
A critical component of the acute management of pediatric patients with traumatic brain injury is calculating the Glasgow Coma Scale (GCS).
Want to learn more about this topic?
Watch the Osmosis video: Approach to traumatic brain injury (pediatrics): Clinical sciences
References
- (2019). AAP endorsed review on diagnosing and managing pediatric head trauma. AAP. 10.1542/pir.2018-0257
- (2019). Clinical guidelines on managing severe traumatic brain injury. AAP/CNS. 10.1093/neuros/nyz051
- Gelineau-Morel RN, Zinkus TP, Le Pichon JB. Pediatric Head Trauma: A Review and Update. Pediatr Rev. 2019;40(9):468-481. doi:10.1542/pir.2018-0257
- Kochanek PM, Tasker RC, Carney N, et al. Guidelines for the Management of Pediatric Severe Traumatic Brain Injury, Third Edition: Update of the Brain Trauma Foundation Guidelines, Executive Summary. Neurosurgery. 2019;84(6):1169-1178. doi:10.1093/neuros/nyz051
- Babl FE, Borland ML, Phillips N, et al. Accuracy of PECARN, CATCH, and CHALICE head injury decision rules in children: a prospective cohort study. Lancet. 2017;389(10087):2393-2402. doi:10.1016/S0140-6736(17)30555-X
- Carney NA, Chesnut R, Kochanek PM, et al. Guidelines for the acute medical management of severe traumatic brain injury in infants, children, and adolescents. Pediatr Crit Care Med. 2003;4(3 Suppl): S1. doi: 10.1097/01.CCM.0000067635.95882.24
- Kliegman, RM, St Geme, JW, Blum, NJ, et al, eds. Nelson Textbook of Pediatrics. 21st ed. Elsevier; 2020.
- Kochanek PM, Tasker RC, Bell MJ, et al. Management of Pediatric Severe Traumatic Brain Injury: 2019 Consensus and Guidelines-Based Algorithm for First and Second Tier Therapies. Pediatr Crit Care Med. 2019;20(3):269-279. doi:10.1097/PCC.0000000000001737

Want more USMLE® Step 2 CK practice questions? Try Osmosis from Elsevier today! Access your free trial and discover why millions of current and future clinicians and caregivers love learning by Osmosis.
Leave a Reply