

A 25-year-old woman at 30 weeks’ gestation presents with uterine cramping and regular contractions with minimal cervical dilation. Which diagnostic finding best distinguishes preterm labor from threatened preterm labor?
A 25-year-old primigravid woman at 30 weeks estimated gestational age (EGA) presents to Labor & Delivery Triage with cramping and low back pain after a long walk on a scorching summer day. She has had no vaginal bleeding, loss of fluid, or decreased fetal movement. She has received regular prenatal care, and her pregnancy has been uncomplicated. Past medical history is notable for mild intermittent asthma, requiring her rescue inhaler about once per month. Temperature is 36.5°C (97.8°F), pulse is 88/min, respirations are 18/min, and blood pressure is 112/76 mmHg. A sterile speculum exam (SSE) is performed, showing white-clear vaginal discharge without an odor; samples are collected. A sterile vaginal exam (SVE) shows the cervix is < 1 cm dilated and 30% effaced. Initial cardiotocographic monitoring shows a baseline fetal heart rate of 130, moderate variability, no decelerations, and contractions every 3 to 5 minutes.
Which of the following is the best next step in the evaluation?
A. Abdominal ultrasound
B. Send a fetal fibronectin (fFN) sample
C. Wet mount of vaginal secretions
D. Assess the cervical length
E. Urinalysis
Scroll down for the correct answer!
The correct answer to today’s USMLE® Step 2 Question is…
D. Assess the cervical length
Correct: See Main Explanation.
Incorrect Answer Explanations
A. Abdominal ultrasound
Incorrect: The best next step is to sonographically measure the cervical length. However, this measurement should be obtained using an endovaginal, rather than abdominal, ultrasound.
B. Send a fetal fibronectin (fFN) sample
Incorrect: The fFN should only be sent if the diagnosis of preterm labor is uncertain based on the SVE (cervix < 3 cm dilated) and the cervical length (between 20 and 30 mm). Therefore, for this patient, a transvaginal ultrasound should first be performed to assess cervical length.
C. Wet mount of vaginal secretions
Incorrect: Bacterial vaginosis (BV) has been associated with an increased risk of preterm birth in some studies. Testing for BV is indicated in the presence of abnormal discharge, which this patient lacks. Although screening for BV in patients with uterine irritability is reasonable, it is a lower priority than assessing the cervical length.
E. Urinalysis
Incorrect: Urinary tract infections are associated with preterm labor, and a urinalysis should be obtained in all patients undergoing a preterm labor evaluation. However, measuring the cervical length is a higher priority, as it is a key criterion used to diagnose preterm labor.
Main Explanation
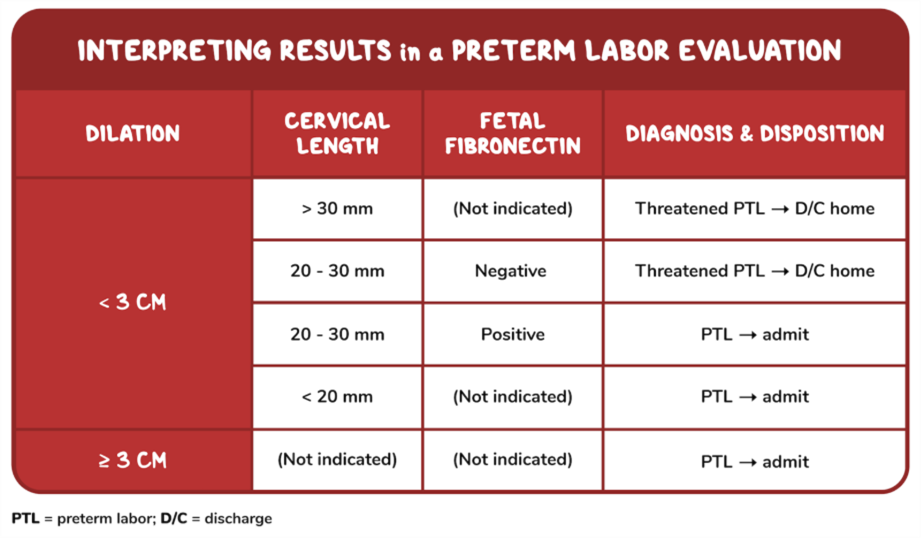
This patient, who presents with cramping, low back pain, and contractions on tocographic monitoring, has symptoms suggestive of possible preterm labor. Preterm labor is defined as regular uterine contractions that cause cervical change between 20 and 36 6/7 weeks EGA. The two most important components of the evaluation are a sterile vaginal exam (SVE) to assess cervical dilation and effacement and, if dilation is < 3 cm, an endovaginal sonographic measurement of the cervical length (CL), which is the most appropriate next step in the vignette where the cervix is < 1 cm dilated.
Preterm labor is diagnosed if the cervix is dilated to ≥ 3 cm and/or the CL is < 20 mm on endovaginal ultrasound. Conversely, preterm labor is ruled out if the cervix is dilated to < 3 cm and the CL is > 30 mm. If the cervix is < 3 cm, but the CL is between 20 and 30 mm, this is an indeterminate result, and an fFN sample should be sent for evaluation.
Additionally, pelvic infections can lead to uterine irritability. Therefore, it is also prudent to obtain a urinalysis and culture in patients with risk factors for sexually transmitted infections, including chlamydia and gonorrhea. A rectovaginal swab should be obtained to screen for group B Streptococcus (GBS), the results of which will affect intrapartum management.
Major Takeaway
The two most important components of a preterm labor evaluation include a sterile vaginal exam to assess cervical dilation and effacement; and, if cervical dilation is < 3 cm, an endovaginal sonographic measurement of the cervical length.
Want to learn more about this topic?
Watch the Osmosis video: Preterm labor: Clinical sciences
References
- American College of Obstetricians and Gynecologists’ Committee on Practice Bulletins—Obstetrics (2016). Practice Bulletin No. 171: Management of Preterm Labor. Obstetrics and Gynecology, 128(4), e155–e164. https://doi.org/10.1097/AOG.0000000000001711

Want more USMLE® Step 2 CK practice questions? Try Osmosis from Elsevier today! Access your free trial and discover why millions of current and future clinicians and caregivers love learning by Osmosis.
Leave a Reply