Acne: Nursing
Acne: Nursing
Watch later
Watch later
Notes
| ACNE | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
| CAUSES AND RISK FACTORS |
| |
| PATHOPHYSIOLOGY |
| |
| SIGNS AND SYMPTOMS |
| |
| DIAGNOSIS |
| |
| TREATMENT |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
Transcript
Acne is a common skin condition in which pores of the skin become blocked by ingrown hair, oil, dead skin cells, or bacteria. It is often linked to hormonal fluctuations in teenagers and young adults, and can sometimes persist into adulthood. Let’s start by quickly reviewing the physiology of the skin. The skin has three main layers: epidermis, dermis, and hypodermis or subcutaneous tissue. The epidermis is the outer layer of the skin that houses cells filled with melanin pigment and keratin, called keratinocytes. Right beneath the epidermis, there’s the dermis, which is a layer of connective tissue that contains the blood vessels and nerves of the skin. Additionally, the dermis also houses epidermal appendages, which are structures that originate from the epidermis but extend into the dermis, such as hair follicles and sebaceous glands.
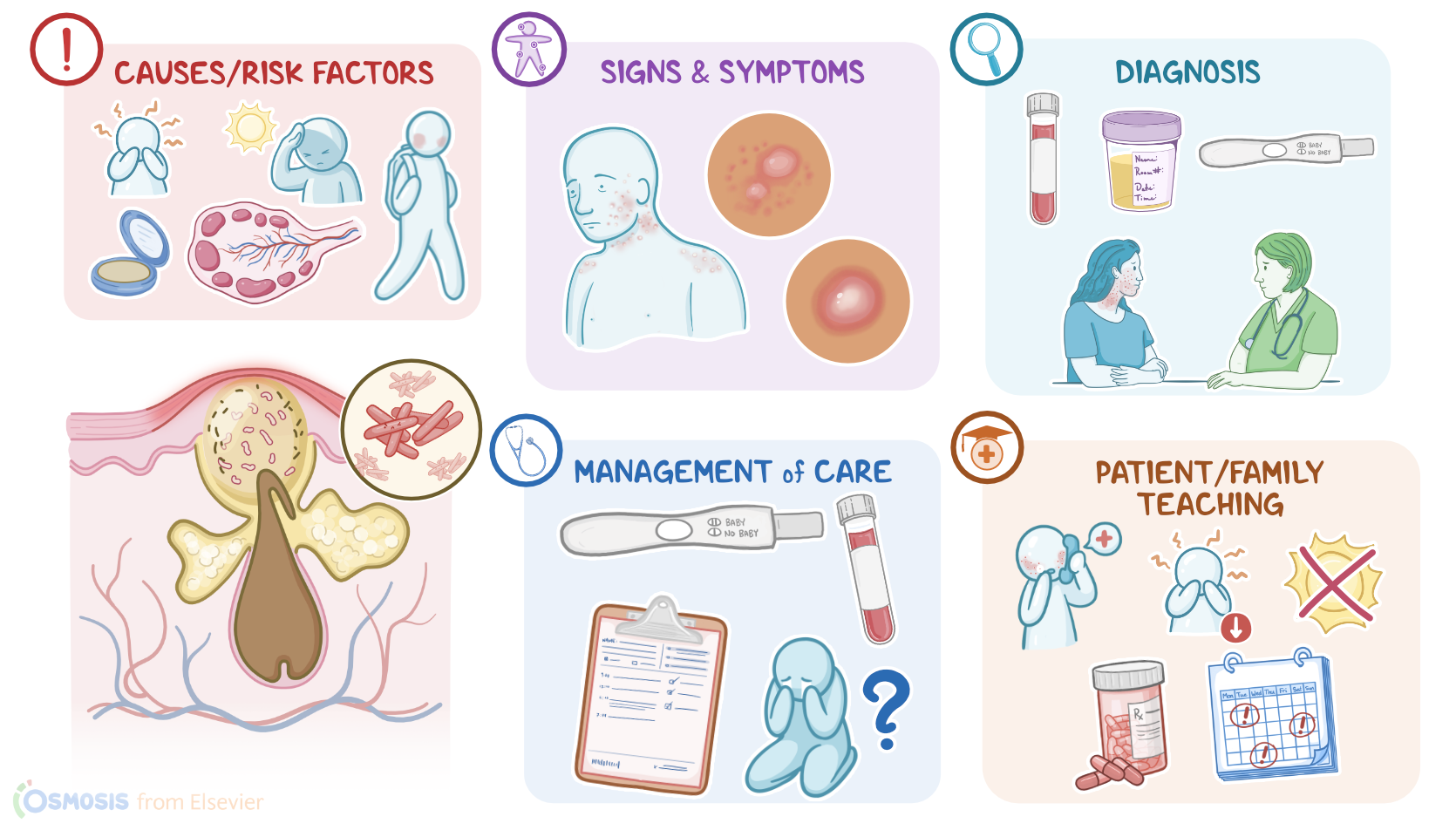
Hair follicles are the living structures of hairs, which are surrounded by a layer of keratinized tissue called the hair shaft. This shaft extends through the epidermis to open into tiny pores on the surface of the skin. Additionally, the sebaceous glands produce oil or sebum under the influence of androgen hormones. Then, it pumps this oil through small ducts that open into the hair shaft at the junction between the epidermis and the dermis. Finally, the dermis is lined on the inside by the subcutaneous tissue, which is a fatty connective tissue that functions in insulation and temperature regulation. All right, so the main cause of acne is blockage of the tiny pores of the skin by dead skin cells, bacteria, and overproduction of sebum by sebaceous glands. When it comes to risk factors of acne, these can be modifiable or non-modifiable. Modifiable risk factors include stress, using oily skin products, steroid use, excessive exposure to sunlight, and repetitive friction or pressure on the skin.
For non-modifiable risk factors, these include family history of acne, as well as younger ages and hormonal changes in puberty and pregnancy. Acne can also affect clients with polycystic ovary syndrome or PCOS, which is characterized by increased androgen levels that cause sebum overproduction; as well as Cushing syndrome, which is when excess cortisol levels overstimulate sebum production. The pathology of acne starts when the small pores of the skin are blocked with sebum or a collection of dead skin cells, called keratin plugs. Acne can be of two types: non-inflammatory and inflammatory. Non-inflammatory acne, also called comedones, are small bumps of the skin that can be closed or open to the surface of the skin. Partially blocked skin pores are called open comedones or black heads. Here, air flows into the pores and oxidizes the melanin of the keratin plugs, which causes them to turn black. On the other hand, completely blocked skin pores are called closed comedones or white heads. Closed comedones doesn’t allow air to flow inside the skin pore, therefore, it provides the perfect environment for growth of anaerobic bacteria, such as Propionibacterium acnes, or P. acnes for short.
Under normal conditions, these bacteria live in the sebaceous glands and hair follicles and don't cause any issues; however, with a complete blockage, the bacteria can proliferate rapidly. This leads to the development of inflammatory acne, when the bacterial overgrowth attracts immune cells, such as neutrophils and macrophages. Typically, this results in the formation of pus, which is a yellowish fluid filled with dead bacteria, immune cells, and tissue debris. Overtime, the accumulating pus produces small bumps on the skin called pustules, which can sometimes combine to form nodules or cysts. The main clinical manifestations of acne include non-inflammatory skin lesions, such as open and closed comedones, as well as inflammatory lesions, such as papules and pustules. These lesions are typically separated and individual, and develop mainly on the face, neck, shoulders, and upper back. Sometimes, comedones can progress into nodules, which are painful elevated masses under the skin that can cause scarring. Some clients may even develop cystic acne, which is characterized by painful, pus-filled lumps or cysts under the skin.
Additionally, clients may present with signs and symptoms of an underlying condition. For example, clients with PCOS could be overweight, they can present with excessive hair growth, and may have menstrual irregularities.On the other hand, clients with Cushing syndrome can have skinny limbs with truncal obesity and abdominal stretch marks, as well as full moon facies or a fatty hump on the upper back, easy bruising, and menstrual irregularities. The diagnosis of acne is based on the client’s history and physical assessment, which are usually sufficient to establish the presence and the severity of acne. Further investigations can be done to establish the underlying cause, like determining serum androgen levels to look for PCOS; or a 24 hour urine collection can be done to measure urinary cortisol levels when Cushing syndrome is suspected. A pregnancy test can also be done when pregnancy is a possibility. Now, the treatment of acne aims at suppressing the development of new lesions and preventing the formation of scars.