Anemia - Iron-deficiency: Nursing
Definitions & Key takeaways
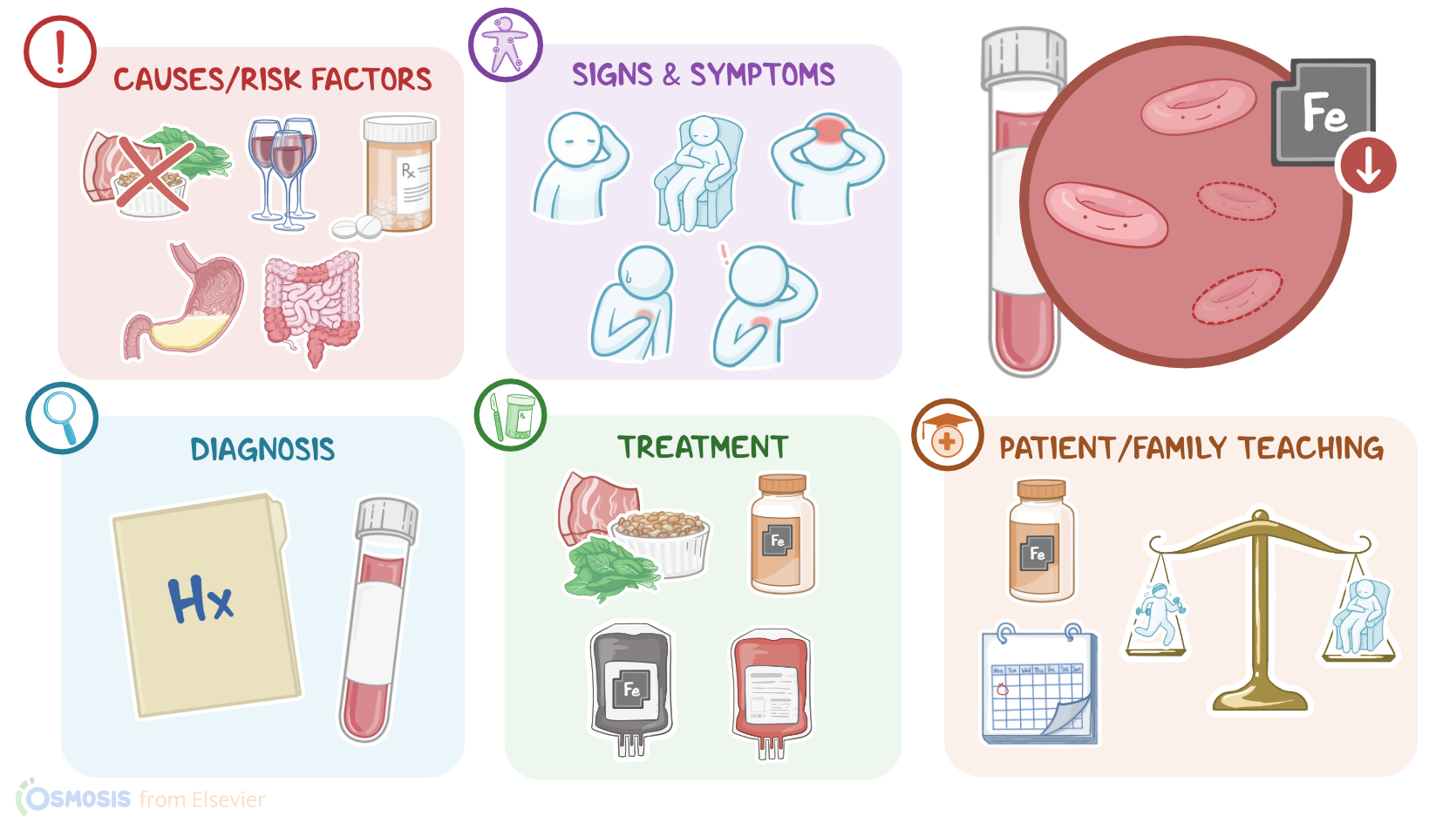
Iron deficiency anemia (IDA) is a condition in which the body is unable to produce sufficient hemoglobin in the red blood cells, due to an inadequate amount of iron in the body. Hemoglobin in the red blood cells is responsible for carrying oxygen throughout the body, so without enough of it, the body doesn't get the oxygen it needs. People with IDA present with symptoms like fatigue, weakness, shortness of breath, and difficulty concentrating. It can also lead to more serious conditions like developmental delay in children, heart failure, and organ damage.
There are several reasons why someone might develop IDA. The most common cause is simply not getting enough iron in your diet. Other causes include bleeding (either internally or externally), chronic illness, and during states in which the body's iron demands are increased such as pregnancy. IDA is characterized by microcytic and hypochromic red blood cells on the peripheral blood smear.
Introduction0:00–0:17
Physiology0:17–1:30
Causes & risk factors1:30–3:10
Pathology3:10–3:57
Clinical manifestations3:57–4:45
Diagnosis4:45–5:51
Treatment5:51–6:11
Management and care6:11–7:43
General client and family teaching7:43–8:30
Review8:30–9:50
| ANEMIA - IRON DEFICIENCY | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
| CAUSES AND RISK FACTORS |
| |
| PATHOPHYSIOLOGY |
| |
| SIGNS AND SYMPTOMS |
| |
| DIAGNOSIS |
| |
| TREATMENT |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
No notes for this video yet
Try adding a note below