Appendicitis: Nursing process (ADPIE)
Client Report0:00–0:26
16 year old Manny Correa is admitted to the pediatric inpatient unit from the urgent care clinic. Manny's father George brought him into the clinic after Manny experienced pain around his belly button for the past 24 hours.
An abdominal ultrasound confirmed an inflamed appendix. Manny is scheduled for an appendectomy today.
Pathology0:26–4:12
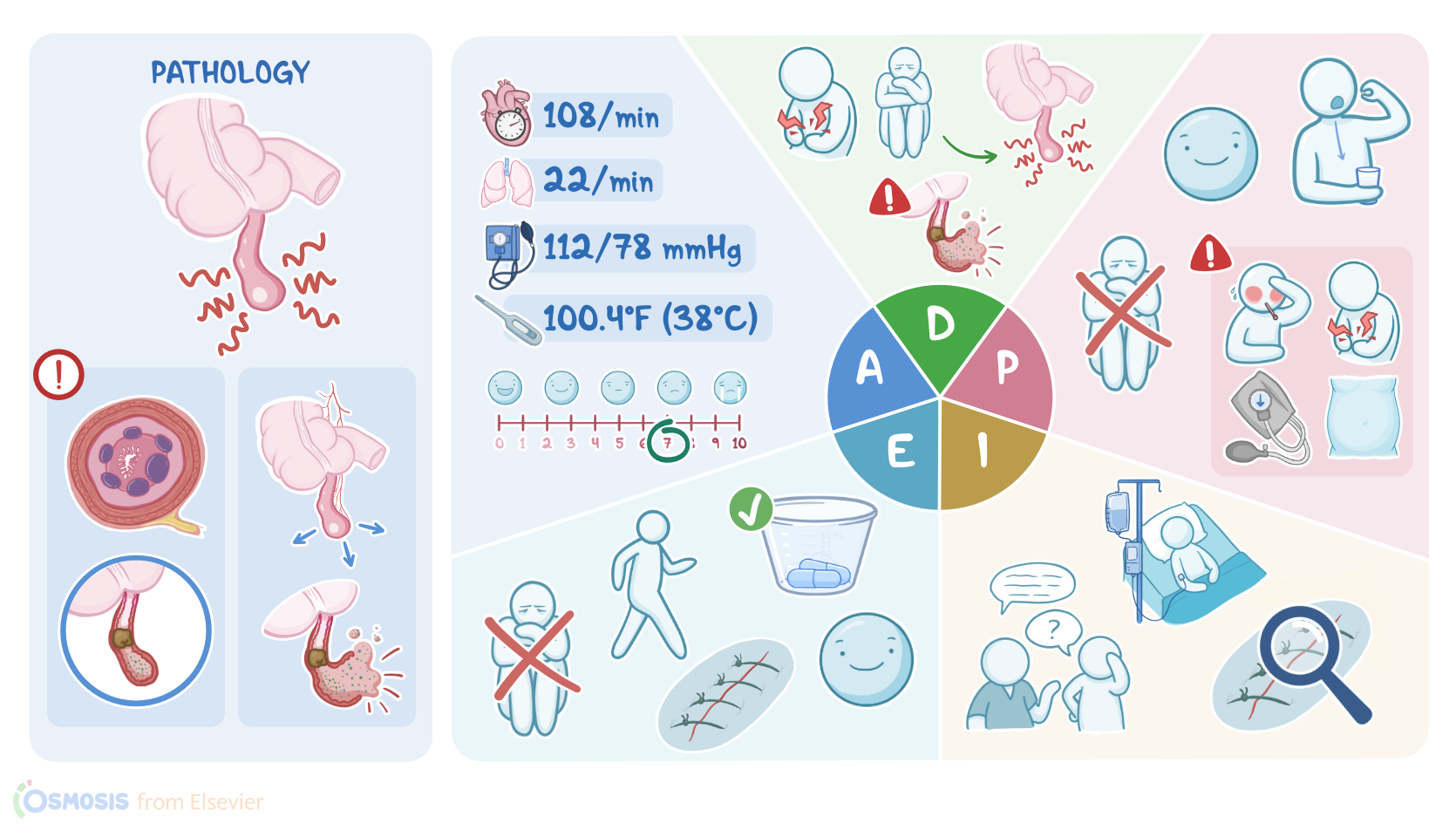
Appendicitis is a condition where the appendix, a finger-like projection that hangs off the cecum of the large intestine, becomes obstructed and inflamed.
Appendicitis can be caused by lymphoid hyperplasia, where overgrown lymphoid follicles obstruct the appendix, or when a hard lump of stool called a fecolith, a tumor, or even parasites like pinworms cause an obstruction resulting in appendicitis.
Appendicitis is more common in the 2nd and 3rd decades of life, with the highest incidence between the ages of 10 and 19, and it's more common in men than in women.
Now when the appendix becomes obstructed, mucosal secretions and the bacteria that normally live in the appendix build up inside, causing the appendix to expand and press against the visceral nerve fibers, resulting in pain that's often felt in the perambilical area.
Eventually, the appendix starts to irritate the nearby parietal membrane lining the walls of the abdominal cavity, causing the pain to intensify and migrate to the lower right quadrant, an area known as McBurney's Point, which is located 1.5 to 2 inches from the navel to the anterior superior iliac spine.
Palpating McBurney's point and quickly releasing pressure will demonstrate rebound tenderness, and the person may show guarding where their abdominal muscles tense up when pressed in an attempt to avoid pain.
Rav Singh's sign is elicited if pressure over the person's left lower abdominal quadrant causes pain in the right lower abdominal quadrant.
The psoas sign is when pain occurs with passive extension of the right hip. Lastly, the operator sign is elicited by flexing the right knee to a 90 degree angle while internally rotating the hip.
Complications can develop as the appendix continues to swell and compress the venous and arterial blood flow. This leads to edema, ischemia, and eventually necrosis of the appendiceal wall.
As cells die, the wall becomes weaker and weaker until it eventually ruptures, allowing bacteria, pus, and fluid to escape into the peritoneum.
The result is the formation of abscesses around the appendix or peritoneal inflammation referred to as peritonitis. At first, the person may notice a sudden decrease in pain as the pressure inside the appendix is relieved.
However, as infection and inflammation continues to develop inside the peritoneal cavity, the person can develop severe abdominal pain and rigidity, vomiting, tachycardia, and hypotension.
If untreated, peritonitis can progress to shock or septicemia. After a client history and physical examination is complete, laboratory and other diagnostic tests can help confirm a diagnosis of appendicitis.
Abdominal ultrasound can be used to visualize inflammatory changes. Abdominal CT scans are more sensitive and can show a more precise view of these findings.
An MRI is useful in diagnosing appendicitis in pregnancy or when contrast must be avoided. A CBC will often show leukocytosis with a left shift or an increased number of immature neutrophils.
A C-reactive protein, which is an indication of inflammation is often elevated. Sometimes uncomplicated appendicitis is treated with a course of antibiotics, but the definitive treatment for appendicitis is the surgical removal of the appendix, referred to as an appendectomy.
If an abscess has formed and there's no evidence of peritonitis, treatment may involve draining the abscess with a needle.
Assessment4:12–5:27
After introducing yourself, confirming Manny's identity, and performing hand hygiene, you note that Manny is laying on his right side with his knees drawn up towards his chest.
His vital signs are BP 112/78 millimeters of mercury, heart rate 108 BPM and regular, respiratory rate 22 breaths per minute with clear lung sounds, oxygen saturation, 99% on room air, and tympanic temperature, 100.4 °F or 38 °C.
Manny is 5' 9 inches and weighs 148 lbs. He tells you, first I had pain around my belly button, but now it hurts a lot more on my right side.
He rates his pain as a 7 out of 10 and describes it as a constant aching. He feels nauseated but has not experienced any vomiting.
You review Manny's initial labs and note that his white blood cell count is 13,500 per cubic millimeter with elevated band cells.
After documenting your assessment findings, you let Manny and George know that the physician assistant or PA will be in soon to do a pre-op assessment and obtain surgical consent.
Based on your assessment of Manny, you identify these priority nursing diagnoses to help guide your nursing care, acute pain related to inflammation of the appendix, nausea related to inflammation of the appendix, risk for infection related to possible rupture of the appendix and surgical incision, and risk for delayed surgical recovery.
Diagnosis5:27–5:47
Planning5:47–6:29
Now it's time to collaborate with Manny's healthcare team to develop a plan of care. Your goals for Manny are that his pain will be managed pre and post-operatively at a stated level of 3 out of 10.
Before discharge, he will report an absence of nausea, he will tolerate oral intake, he'll remain free of signs and symptoms of infection, and he will not experience other post-operative complications such as pneumonia, clot formation, or paralytic ileus.
As you continue to monitor Manny, you will alert the healthcare team for changes that indicate rupture, abscess formation, or peritonitis, such as a drop in BP, high fever, rigid abdomen, or severe pain.
Implementation6:29–7:18
After identifying Manny's goals, you can start to implement the plan of care. You initiate IV fluids along with parenteral antibiotics, analgesics, and antiemetics, and you explain to Manny and George that he is now NPO for surgery.
Next, you assist Manny to sit in a semi-fowler's position with pillows under his knees to reduce tension on the abdominal wall.
Finally, you explained that after surgery, his pain will be managed and how his surgical incision will be monitored for bleeding and infection.
You provide teaching about preventing post-operative pulmonary complications through deep breathing and coughing while splinting his abdomen and discuss the need to be up and walking soon after surgery to help prevent problems like constipation, ileus, and deep vein thrombosis.
Manny has had a successful laparoscopic appendectomy and is transferred back to the pediatric inpatient unit. His vital signs are BP 110/80 millimeters of mercury, heart rate 88 BPM and regular, respiratory rate 16 breaths per minute with clear lung sounds, oxygen saturation, 98% on 2 L of oxygen per nasal cannula, and tympanic temperature of 98.8 °F or 37.1 °C.
Evaluation7:18–8:30
He rates his pain as 2 out of 10, his bowel sounds are active, and he says he's not nauseous. He asks you if he can have something to drink.
After bringing Manny a cup of water, you remind him to start slowly with his oral intake. You take a moment to review the postoperative teaching you provided before surgery.
George tells you that he plans on helping Manny walk down the hall and back soon. Manny will stay overnight and be discharged tomorrow as long as he is afebrile, tolerating oral intake, his vital signs are stable, his pain is controlled, and his incisions are clean, dry and intact.
You and your team will continue reevaluating his plan of care during his hospital stay. All right, as a quick recap, 16 year old Manny was diagnosed with appendicitis, a condition in which the appendix becomes obstructed and inflamed.
Summary8:30–9:15
Your assessment of Manny revealed a low-grade fever, pain, and nausea. The nursing diagnoses you identified for Manny are acute pain, nausea, risk for infection, and risk for delayed surgical recovery.
Goals you identified when planning care with Manny's healthcare team included management of Manny's pain and nausea and preventing post-operative complications.
With the help of Manny's healthcare team and his dad, George, you implemented strategies to reach these goals. Afterwards, you evaluated if Manny's goals were met.
While you care for Manny, you will continue reevaluating his plan of care using the nursing process.
| APPENDICITIS | ||
| KEY POINTS | NOTES | |
| PATIENT REPORT |
| |
| PATHOPHYSIOLOGY |
| |
| ASSESSMENT |
| |
| NURSING DIAGNOSES |
| |
| PLANNING |
| |
| IMPLEMENTATION |
| |
| EVALUATION |
| |
- "Ackley and Ladwig’s Nursing Diagnosis Handbook: An Evidence-Based Guide to Planning Care, 13th edition" Mosby (2022)
- "Post operative pediatric appendicitis nurse-driven discharge: Patient outcomes and nursing perspectives" Am J Surg (2021)
- "Appendicitis in a ventral hernia" Visual Journal of Emergency Medicine (2023)
- "Medical-Surgical Nursing: Concepts for Interprofessional Collaborative Care, 10th Edition" Elsevier (2020)
- "Harrison’s Principles of Internal Medicine, 21st edition" McGraw Hill / Medical (2022)
- "Simultaneous occurrence of acute appendicitis and appendicular band syndrome in a patient with intestinal obstruction" Visual Journal of Emergency Medicine (2023)
- "Routine post-operative labs and healthcare system burden in acute appendicitis" Am J Surg (2023)
- "Health Assessment for Nursing Practice, 7th edition" Elsevier (2021)
No notes for this video yet
Try adding a note below