Arrhythmias - Ventricular tachycardia (Vtach): Nursing
1,003views
Notes
| ARRHYTHMIAS - VENTRICULAR TACHYCARDIA (VTACH) | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
| CAUSES AND RISK FACTORS |
| |
| PATHOPHYSIOLOGY |
| |
| SIGNS AND SYMPTOMS |
| |
| DIAGNOSIS |
| |
| TREATMENT |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
Transcript
Arrhythmias are irregular heartbeats that occur due to any disturbance in the rate, rhythm, site of origin, or conduction of the cardiac electrical impulse, which can affect the heart’s ability to pump blood throughout the body.
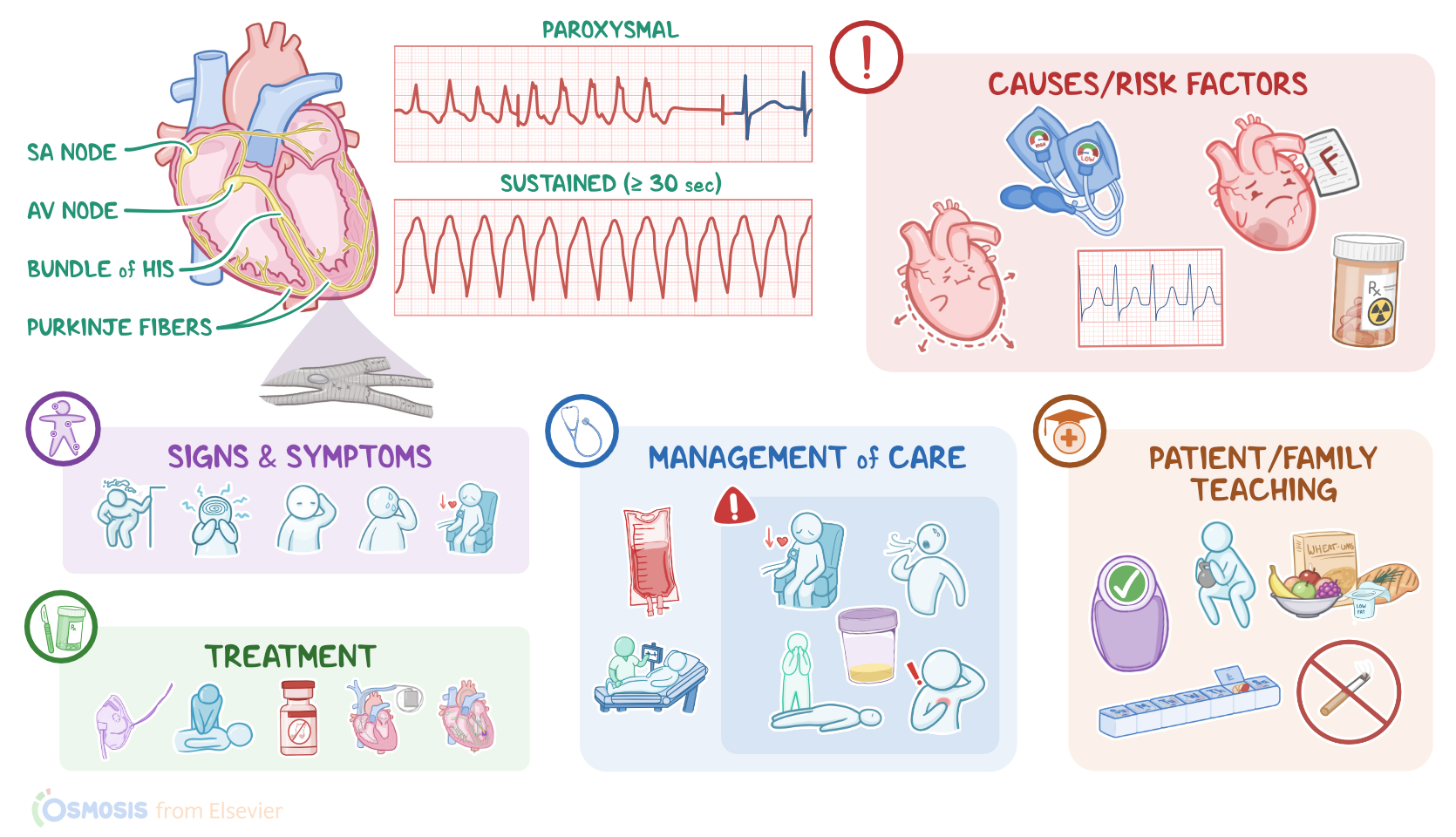
Ventricular tachycardia, or simply V-tach, is a type of tachyarrhythmia, where a point in the ventricles fires abnormal signals, causing the heart to beat faster than normal, at a rate of 150 to 250 beats per minute. Ventricular tachycardia can be paroxysmal, meaning that it presents as three or more beats that are self-limiting; or sustained, meaning that it lasts for at least 30 seconds.
Now let’s look at the normal electrical conduction pathway in the heart on an ECG, which shows how the depolarization wave flows through the heart during each heartbeat. The normal electrical activity of the heart starts in the sinoatrial or SA node, which is considered the pacemaker of the heart. Then, the impulse is conducted through the atrium, creating the P wave on an ECG. And when the atrial muscle cells get depolarized, they contract, pushing blood from the atria into the ventricles. From the atrium, electrical activity goes to the atrioventricular, or AV node, where the impulse propagation speed slows way down; this is the PR interval on an ECG. This pause allows the atria to contract while the ventricles fill with blood. From the AV node, the depolarization wave goes through the Bundle of His, then the right and left branches of the Bundle, and finally through the Purkinje fibers, which deliver the current to
the right and left ventricles, causing them to depolarize. This triggers simultaneous contraction of both ventricles, pushing blood into the systemic and pulmonary circulations, and it’s represented by the QRS complex on an ECG. Finally, the ventricles repolarize to prepare for the next cycle, which allows them to relax and fill with blood, called diastole. And on ECG, ventricular repolarization will create a T wave, while the pause between ventricular depolarization and repolarization is represented by the ST segment. Sometimes, immediately after the T wave, there’s a U wave, which represents late repolarization of the ventricles.
Okay, now back to ventricular tachycardia, which is typically caused by any kind of structural damages to the heart that lead to electrical changes in the heart muscle cells. These changes are strongly associated with several risk factors, particularly certain heart conditions. These include ischemic heart disease, previous or recent myocardial infarction, in addition to cardiomyopathy, supraventricular tachycardia, valvular heart disease, and heart failure.
In addition, clients with electrolyte imbalances, such as hypokalemia and hypomagnesemia, as well as chronic obstructive pulmonary disease, or COPD, are at an increased risk for ventricular tachycardia. Finally, other risk factors include hyper- and hypotension, as well as drug toxicity, typically with steroids; in addition to cocaine and inhalants use.
Now, the pathology of ventricular tachycardia starts when any of these factors stress or damage the ventricular muscle cells, which can lead to ectopic nodal automaticity or reentrant signaling. Ectopic nodal automaticity suggests that a ventricular cell, called a ventricular ectopic focus, starts firing at higher rates that exceed the rate of the firing of the SA node, which increases the heart rate to more than 150 beats per minute. What messes things up is that the SA node may continue to send off signals, causing contraction of the atria that is independent of the contraction of the ventricles.
On the other hand, reentrant signaling happens when a depolarization wave encounters tissue that doesn’t depolarize, which could be due to the presence of scar tissue after myocardial infarction. Here, the wave starts going around and around that tissue, forming what’s called a reentrant loop. Ultimately, these mechanisms cause irritability of ventricular cells, which leads to ventricular tachycardia.
When it comes to complications of ventricular tachycardia, these include hypotension, pulmonary edema, decreased cerebral blood flow, as well an increased risk of developing ventricular fibrillation, which can lead to a sudden cardiopulmonary arrest or sudden death.
Clients with ventricular tachycardia typically present with dizziness, altered mental status, pallor, as well as diaphoresis, and hypotension. Clinical manifestations can also include chest pain, palpitations, and shortness of breath. Additionally, clients with ventricular tachycardia may or may not have a pulse.