Atopic dermatitis: Nursing process (ADPIE)
Atopic dermatitis: Nursing process (ADPIE)
2144 final exam
2144 final exam
Notes
| ATOPIC DERMATITIS | ||
| KEY POINTS | NOTES | |
| PATIENT REPORT |
| |
| PATHOPHYSIOLOGY |
| |
| DIAGNOSIS AND TREATMENT |
| |
| ASSESSMENT |
| |
| NURSING DIAGNOSES |
| |
| PLANNING |
| |
| IMPLEMENTATION |
| |
| EVALUATION |
| |
Transcript
Kameron Jones is a 2-year-old male who presents to your pediatric clinic accompanied by his mother.
Mrs. Jones explains that Kameron has developed a red rash on his scalp, cheeks, and chest that has gotten worse over the past week.
Yesterday, she noticed that some of those areas of skin looked red and developed cracks that began to ooze.
She says Kameron has been scratching at his chest constantly, and he’s been more irritable, since the rash appeared.
The pediatrician diagnoses atopic dermatitis, and Kameron will begin treatment today.
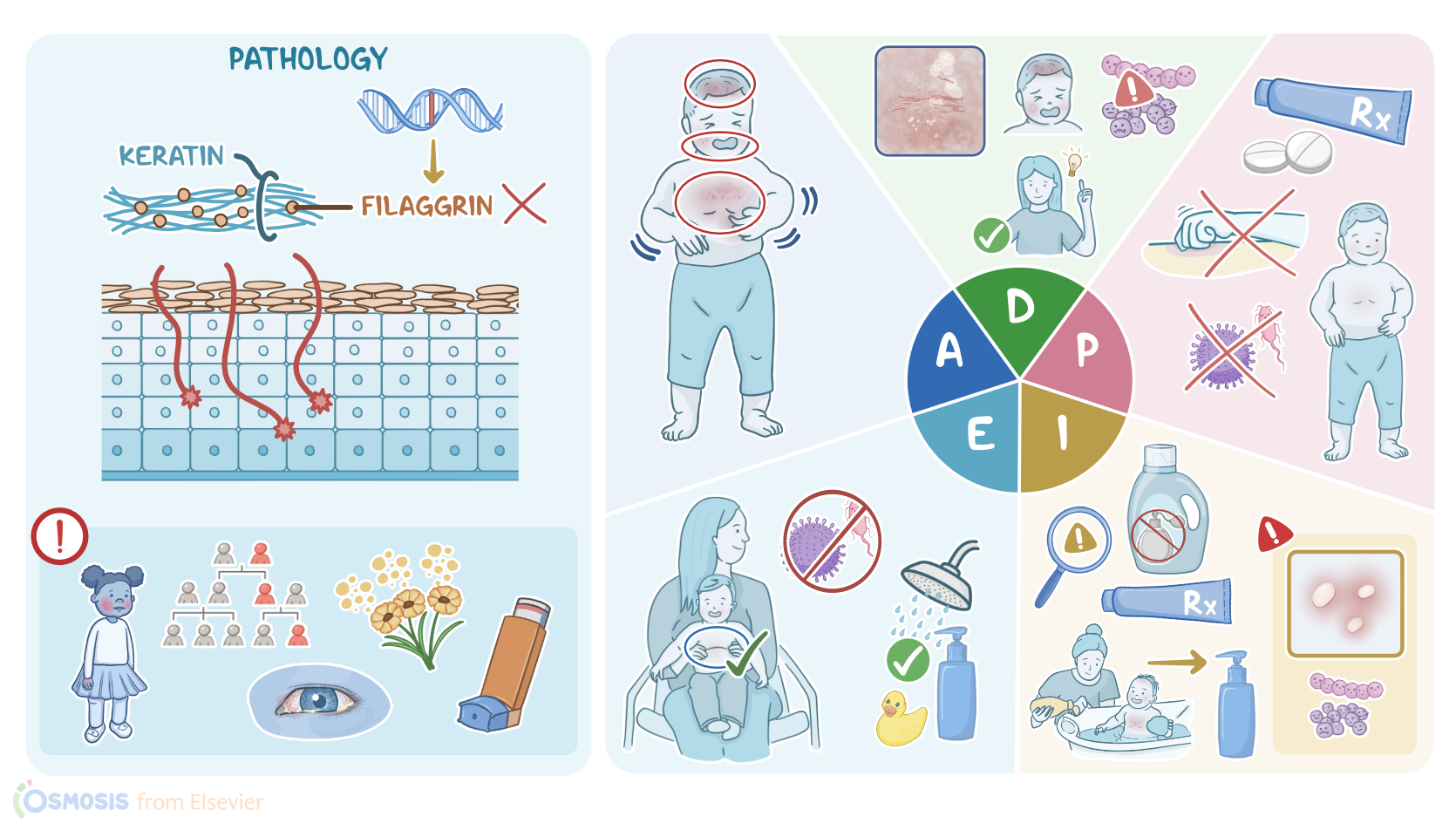
Atopic dermatitis, also known as eczema, is a chronic inflammatory skin disease that occurs most frequently in children, ages five and under, but may also affect adults, especially those with a predisposition towards allergic diseases, including asthma, allergic rhinitis, and conjunctivitis.
Now, the exact cause of atopic dermatitis is not fully understood, however it seems to be a mix of skin barrier abnormalities and dysfunction in the immune system.
In regards to skin barrier abnormalities, atopic dermatitis is associated with a mutation in the filaggrin gene.
Filaggrin is a protein that binds to keratin and contributes to the formation of the skin barrier, so individuals with atopic dermatitis have a slightly porous skin barrier, which sets them up for allergens or microbes to get under the skin.
In regards to dysfunction in the immune system, atopic dermatitis is associated with atopy, which is a genetic predisposition to develop allergies due to an increased inflammatory response to triggers, such as allergens or irritant substances.
There are some risk factors for atopic dermatitis.
Unfortunately, some of them are non-modifiable, including younger age, atopy, family history, and mutations in the filaggrin gene.
On the other hand, modifiable risk factors include contact with triggers, including allergens like pollen, mold, or animal dander, as well as a certain kind of soap or detergent, or an irritant like tobacco smoke.
Clients with eczema typically present with dry, scaly skin that’s very itchy, as well as patches of red, swollen, and easily irritated skin, especially on the face and scalp, but sometimes also on the insides of the elbows or the back of the knees.
When scratched, these sensitive patches of skin may develop erosions, oozing, and crusting.
An important complication that may affect this disrupted skin barrier is secondary bacterial infections, especially staphylococcal and streptococcal infections, but also fungal infections, such as tinea, and viral infections, most often from herpes simplex virus.
Diagnosis of atopic dermatitis is based on the client’s history and physical exam.
Laboratory tests may show increased eosinophils and serum IgE levels, while allergy testing can help identify the specific allergens that should be avoided.
There is no cure for atopic dermatitis, so treatment aims at reducing the symptoms by keeping the skin hydrated with moisturizers, minimizing itching with oral antihistamines, and dampening the inflammatory reaction with topical medications, such as steroid creams like hydrocortisone or calcineurin inhibitors like tacrolimus.
Finally, clients should try to avoid exposure to triggers. Let’s get back to assess Kameron and see how he’s doing.
You wash your hands, introduce yourself to him and his mother, and confirm his identity.
Kameron is sitting in his mother’s lap and appears uncomfortable as he scratches his chest through his shirt.
You ask Mrs. Jones when she first noticed the rash.
She says it appeared on his chest about a week ago, and that she thought something had scratched him, but now that it’s also affecting his face and scalp.
She’s concerned it is getting worse and wonders if it is contagious.
Sources
- "Ackley and Ladwig’s Nursing Diagnosis Handbook: An Evidence-Based Guide to Planning Care, 13th edition" Mosby (2022)
- "Pathophysiology of atopic dermatitis: Clinical implications" Allergy Asthma Proc (2019)
- "Harrison’s Principles of Internal Medicine, 21st edition" McGraw Hill / Medical (2022)
- "Daily Moisturization for Atopic Dermatitis: Importance, Recommendations, and Moisturizer Choices" The Journal for Nurse Practitioners (2021)
- "Molecular Mechanisms of Atopic Dermatitis Pathogenesis" Int J Mol Sci (2021)
- "Critical Care Nursing: Diagnosis and Management, 9th edition" Elsevier (2021)
- "Health Assessment for Nursing Practice, 7th edition" Elsevier (2021)