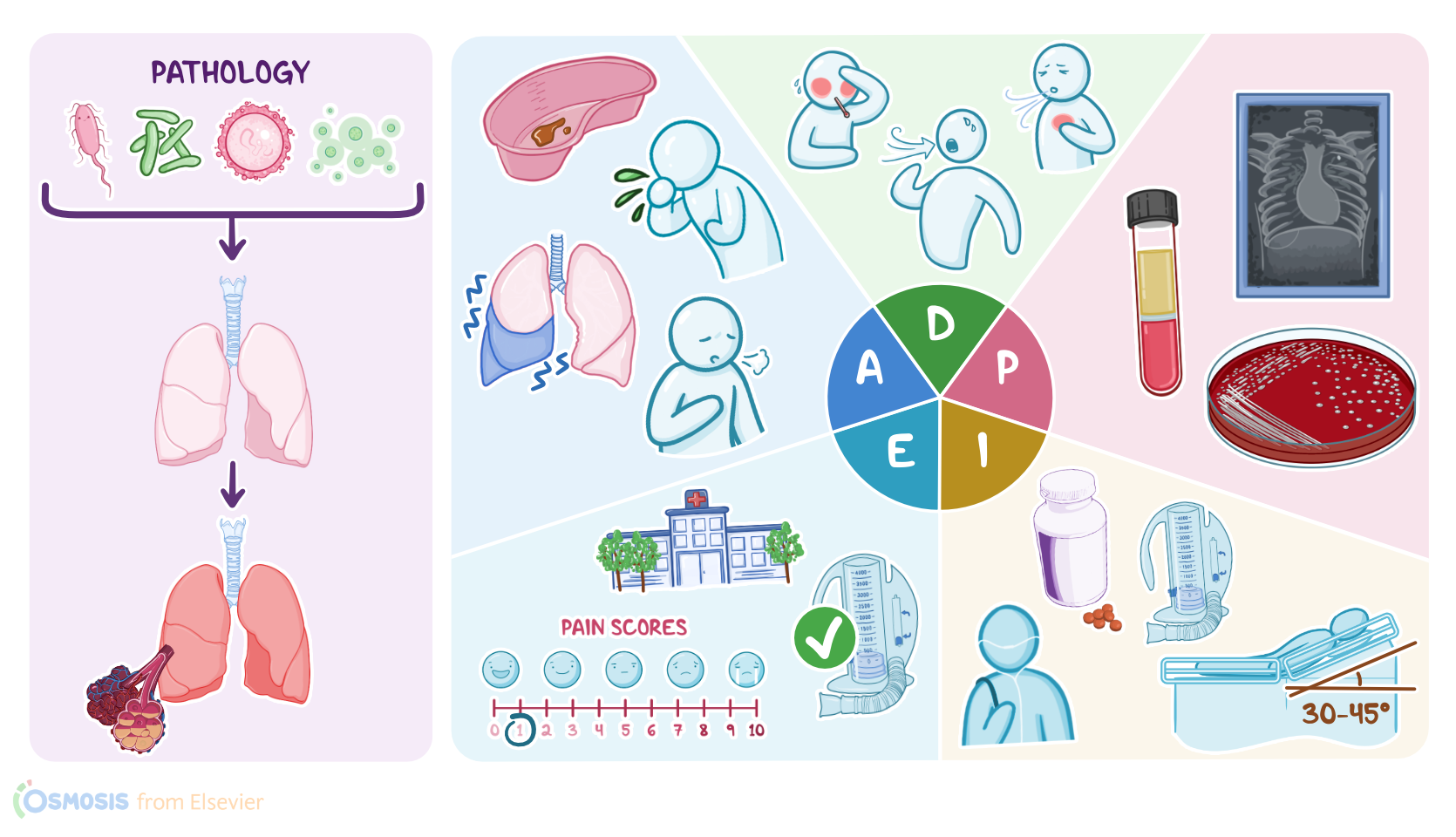
Bacterial pneumonia: Nursing process (ADPIE)
1,514views
Bacterial pneumonia: Nursing process (ADPIE)
Nursing
Nursing
Notes
| BACTERIAL PNEUMONIA | ||
| KEY POINTS | NOTES | |
| PATIENT REPORT |
| |
| PATHOPHYSIOLOGY |
| |
| DIAGNOSIS AND TREATMENT |
| |
| ASSESSMENT |
| |
| NURSING DIAGNOSES |
| |
| PLANNING |
| |
| IMPLEMENTATION |
| |
| EVALUATION |
| |
Transcript
Neli Singh is an 82-year-old man who arrives at the urgent care clinic with his home health aide. Mr. Singh has a history of cardiac disease, type I diabetes, prostate cancer, and depression. He was brought to the clinic this afternoon because of a new onset of a productive cough, dyspnea and chest pain. Mr. Singh’s aide tells the triage nurse, “Neli had these same symptoms 2 months ago. I’m worried its pneumonia again.”
Pneumonia is an infection in the lung tissue caused by microbes, resulting in inflammation. The inflammation brings fluid into the lung tissue, and that extra fluid can make it hard to breathe.
Now, there are lots of different pneumonia-causing microbes. Usually, it’s caused by viruses and bacteria, but it can also be caused by fungi and a special class of bacteria called mycobacteria. In adults, the most common viral cause of pneumonia is influenza, sometimes just called the flu. In adults, bacterial causes include Streptococcus pneumoniae, Haemophilus influenzae, and Staphylococcus aureus. There are also more unusual bacteria like Mycoplasma pneumoniae, Chlamydophila pneumoniae, and Legionella pneumophila, which don’t have a cell wall and are well known for causing an “atypical or walking pneumonia” because they often cause vague symptoms. For example, you might manifest with symptoms of a common cold, and these aren’t severe enough to require you to stay home or be hospitalized. So, you can still be out and about, walking around.
In individuals with a normal immune system, fungi are a rare cause of pneumonia and often it’s regional - for example, there’s Coccidioidomycosis in California and the Southwest. One special fungal culprit is Pneumocystis jiroveci which is a risk for immunocompromised individuals. Finally, there’s mycobacteria which are slow growing like fungi, hence the “myco” in their name even though they’re still bacteria. The most well-known one is Mycobacterium tuberculosis, also just called TB.
Pneumonia can also be categorized by how it’s acquired. The most common is community-acquired pneumonia, and it’s called that when a person gets sick outside of a hospital or other healthcare setting. Next is hospital-acquired pneumonia or nosocomial pneumonia, which is when a person gets pneumonia when they are already hospitalized for something else. This type tends to be more serious because sick clients often have weakened immune systems and the microbes in hospitals are often resistant to common antibiotics. That’s because hospitals bring together the bacteria that are often the most virulent - think great offense - as well as the most resistant - think great defense.
Another category of pneumonia is ventilator-associated pneumonia,
which is a subset of the hospital-acquired pneumonia, that can specifically develop in ill individuals who are connected to a ventilator. Oftentimes, there’s a biofilm - which is a mix of bacteria and sugars and proteins that can coat a surface - that forms on the endotracheal tube. Individuals on a ventilator can’t cough effectively, have limited mobility, and are often quite sick already, so over time microbes can move from the tube directly into the lung and cause pneumonia.
Now in addition to inhaling microbes there are other ways to develop pneumonia. Think about this: you’re eating some French fries, and instead of swallowing one, you accidentally breathe it in. Informally we call that going down the wrong pipe, but we could also say that you aspirated that French fry. Normally, you’d automatically gag and start coughing and work that French fry out of your airway. These gag reflexes can be compromised, however, by drug and alcohol abuse, brain injuries, or swallowing issues. So, in these cases the French fry might stick around in your lower airways. Now, of course, that French fry isn’t sterile, so there might be some microbes stuck to it. If those microbes infect the lungs and you get pneumonia, we call it aspiration pneumonia. Aspiration pneumonia can also happen with drinks, or even gastric contents, like after a bout of vomiting. Aspirated gastric contents can be particularly nasty because the stomach acid can cause a chemical irritation in addition to the possible infection.
So, after you greet Mr. Singh, introduce yourself as his nurse, and confirm his identity, you can’t help but notice the sound of a very productive cough when you enter the room!. Neli, as he’s asked you to call him, says, “I’m glad you’re here! I’ve got lots of phlegm coming up.” You pass Neli the emesis basin from the counter and proceed with your assessment. You first ask how he’s feeling, to which he replies, “Not too bad today, just this cough and a little chest pain, still. Much better than I was before. I was having such a hard time breathing and couldn’t finish a sentence without running out of air.” You wash your hands and listen to Neli’s breath sounds and note rhonchi and wheezing in the right middle and lower lobes, and you feel tactile fremitus - which is when you can feel increased vibrations from a person’s chest or back after they repeat certain phrases. This is because sound travels better through the fluid-filled consolidated tissue than air-filled healthy tissue. As you assess his respiratory rate, you peek over into the emesis basin and observe thick, dark colored sputum inside. Next, you collect his vital signs: HR 105, RR: 22, BP: 138/90, oral temp.: 101.8° F., pain: 4/10, oxygen saturation: 90% on room air. Neli’s aide shares that he’s been a little confused these days - repeating himself and forgetting what he’s doing - adding to her concern that he’s not well. You document all your assessment findings before leaving the room and update Neli and his aide that the Advanced Practice Nurse Practitioner, or APRN, will be in shortly to examine him further.
"not too bad today~ cough~ chest painbefore~ hard time breathing~ couldn't finish sentence w/o runningout of air."
Based on the assessment data you’ve collected; you identify that Neli is at risk for a few problems. These include ineffective airway clearance related to increased production and viscosity of sputum, pain related to his excessive coughing, activity intolerance related to impaired respiratory function, impaired gas exchange related to fluid consolidation in his lungs, and deficient fluid volume related to fever and increased rapid respiratory rate.
Sources
- "Nursing Diagnosis Handbook: An Evidence-Based Guide to Planning Care. 13th edition. ISBN: 978-0-323-77683-7 " Mosby (2022.)
- "Community-acquired bacterial pneumonia in adults: An update. " Indian J Med Res. (2020;151(4):287-302. )
- "Guidelines for the Evaluation and Treatment of Pneumonia. " Prim Care. (2018;45(3):485-503. )
- "Host-Pathogen Interactions in Gram-Positive Bacterial Pneumonia. " Clin Microbiol Rev. (2019;32(3):e00107-18. Published 2019 May 29. )
- "Emerging antibiotics for community-acquired pneumonia [published correction appears in Expert Opin Emerg Drugs. 2019 Dec;24(4):i]. " Expert Opin Emerg Drugs. (2019;24(4):221-231. )
- "Harrison’s Principles of Internal Medicine. 21st edition. ISBN: 978-1-264-26850-4 " McGraw Hill / Medical (2022)
- "Critical Care Nursing: Diagnosis and Management. 9th edition. ISBN: 978-0-323-64295-8 " Elsevier (202)