Bronchiolitis and respiratory syncytial virus (RSV): Nursing process (ADPIE)
1,804views
Bronchiolitis and respiratory syncytial virus (RSV): Nursing process (ADPIE)
Nursing
Nursing
Notes
| BRONCHIOLITIS AND RESPIRATORY SYNCTIAL VIRUS (RSV) | ||
| KEY POINTS | NOTES | |
| PATIENT REPORT |
| |
| PATHOPHYSIOLOGY |
| |
| DIAGNOSIS AND TREATMENT |
| |
| ASSESSMENT |
| |
| NURSING DIAGNOSES |
| |
| PLANNING |
| |
| IMPLEMENTATION |
| |
| EVALUATION |
| |
Transcript
Charlie Santos is a 2-month-old male who is brought to urgent care by his mother. She says that he has had a runny nose and an axillary temperature of 100.4 F, or 38 C, for the past two days.
This morning she noticed that he seemed to need to work harder to breathe, and she tells you he has been fussy and not feeding well. She also mentions that he attends daycare, and recently many of the children have been sick with similar symptoms.
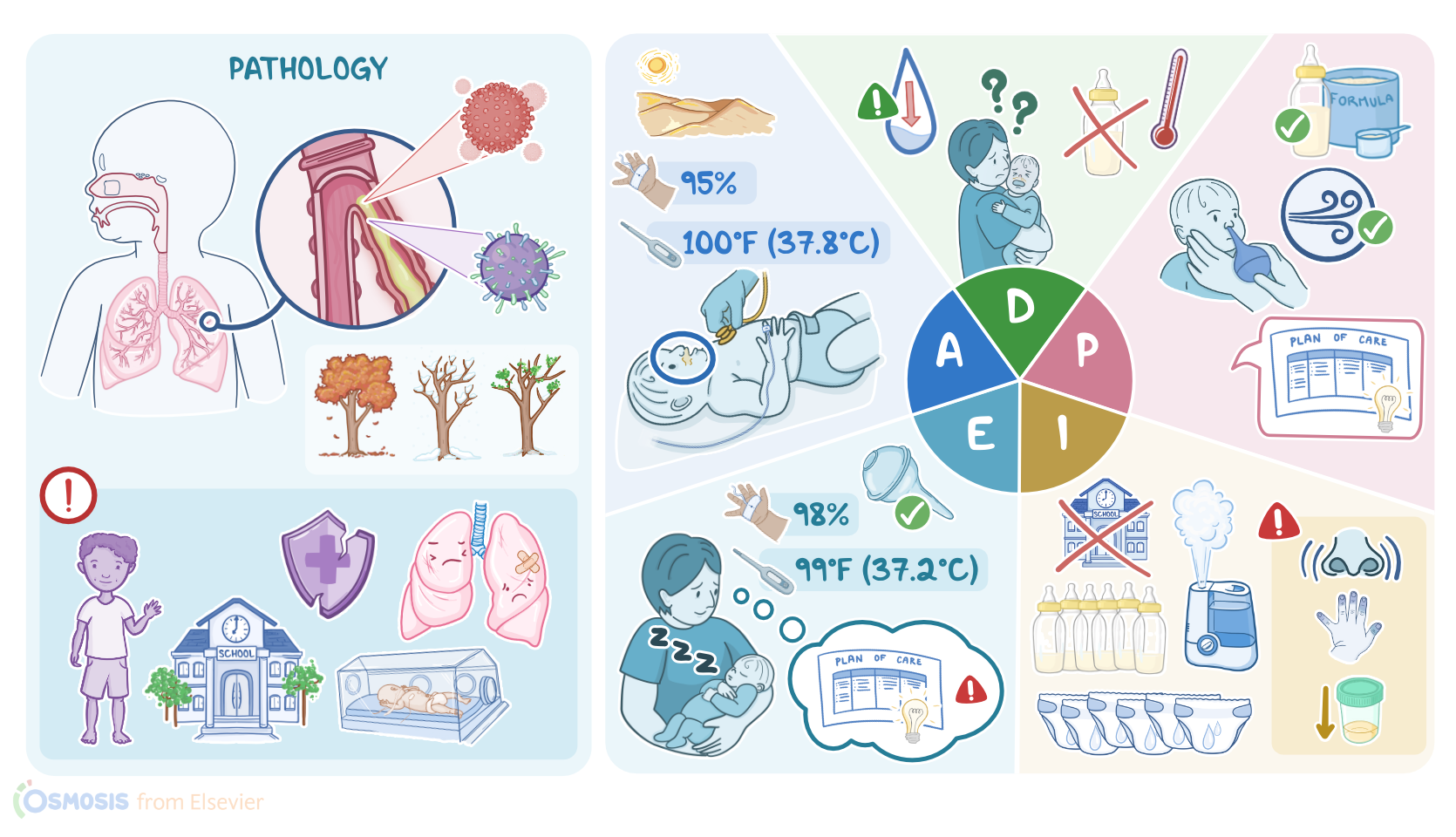
Based on Charlie’s clinical presentation and history, an infection with respiratory syncytial virus, or RSV, is suspected. The respiratory tract is divided into two parts; the upper airway, which consists of the nasal cavity, paranasal sinuses, pharynx, and larynx; and the lower airway, which consists of the trachea, bronchi, bronchioles, alveoli, and lungs.
Inflammation of the bronchioles, which are the smallest airways of the lungs, is known as bronchiolitis. It commonly occurs during the colder months, so fall, winter, and early spring, and it’s most often caused by the respiratory syncytial virus, or RSV for short.
Other causes include viruses like adenovirus, parainfluenza virus, or rarely from bacteria like Mycoplasma pneumoniae. Now, the most important risk factor for bronchiolitis is young age, since it mostly affects children under 2 years of age, with infants less than 3 months being at the highest risk.
Other risk factors include premature birth, attending crowded places like daycare, or having older siblings who can catch it in school. Finally, some underlying conditions may increase the risk of bronchiolitis, including chronic lung disease, congenital heart disease, or being immunocompromised.
Transmission of RSV typically occurs from direct contact with respiratory droplets when an infected person talks, sneezes, or coughs. These droplets can then land in the mouths or noses of people nearby, or be inhaled into their lungs.
The virus can also survive on surfaces for a few hours, so it’s possible to get the virus by touching an infected surface, like a contaminated doorknob, and then touch their own eyes, nose, or mouth.
Now, once the virus has entered the body, it travels down the respiratory tract to the bronchioles and invades its epithelial cells, turning them into a virus factory, and ultimately killing them.
The viral invasion attracts immune cells, which cause an inflammatory reaction that leads to swelling and narrowing of the airway, as well as increased mucus production.
The mucus, along with the dead epithelial cells, creates a plug that can obstruct the airway and cause the alveoli to deflate, leading to atelectasis. The plug can also allow air to enter the lungs via inhalation, but not leave via exhalation.
As a result, the lungs become more inflated with each inhalation, known as air-trapping. Symptoms of bronchiolitis are similar to the common cold, including low-grade fever, congestion, rhinorrhea, and cough.
If the disease progresses, the child may experience dyspnea and tachypnea, and can present wheezing, crackles, and diminished breath sounds.
In severe cases, the child can become lethargic, irritable, and present with poor feedings, and dehydration. In addition, the child can experience central apnea, which means that they have short periods of time where they stop breathing altogether.
This can lead to hypoxia, where there is not enough oxygen in the body, and typically presents with cyanosis. Other important complications of bronchiolitis include atelectasis, as well as pneumonia if the infection spreads to the lungs. Ultimately, respiratory failure can develop.
Diagnosis of bronchiolitis is typically based on clinical assessment. However, diagnostic testing to confirm RSV can be done by swabbing secretions from the nasopharynx and running a rapid antigen detection test, or RADT, or a polymerase chain reaction, or PCR, to determine the presence of viral antigens.
If the symptoms worsen, or if there is concern about the development of complications, a chest X-ray can be done. There’s no proven antiviral therapy for bronchiolitis, so treatment is focused on symptoms.
Most cases can be treated at home by making the child more comfortable by using a cool-mist humidifier, keeping the head elevated while awake, instilling saline nose drops and using nasal suction to ease congestion, as well as promoting adequate fluid intake to prevent dehydration.
Smoke can worsen the symptoms of bronchiolitis, so it is important to maintain a smoke free environment. Over-the-counter medications like acetaminophen or ibuprofen can be given to relieve pain and reduce fever.
Sources
- "Ackley and Ladwig’s Nursing Diagnosis Handbook: An Evidence-Based Guide to Planning Care, 13th edition" Mosby (2022)
- "Rhinovirus Type in Severe Bronchiolitis and the Development of Asthma" J Allergy Clin Immunol Pract (2020)
- "Effectiveness of Targeted Interventions on Treatment of Infants with Bronchiolitis: A Randomized Clinical Trial" JAMA Pediatr (2021)
- "Bronchiolitis therapies and misadventures" Paediatr Respir Rev (2023)
- "Harrison’s Principles of Internal Medicine, 21st edition" McGraw Hill / Medical (2022)
- "Bronchiolitis" CMAJ (2022)
- "Recent advances in the understanding of bronchiolitis in adults" F1000Res (2020)
- "Critical Care Nursing: Diagnosis and Management, 9th edition" Elsevier (2021)