Chest tube care: Nursing
2,491views
Notes
| CHEST TUBE CARE | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
| CHEST TUBES AND DRAINAGE SYSTEMS |
| |
| PROCEDURE |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
Transcript
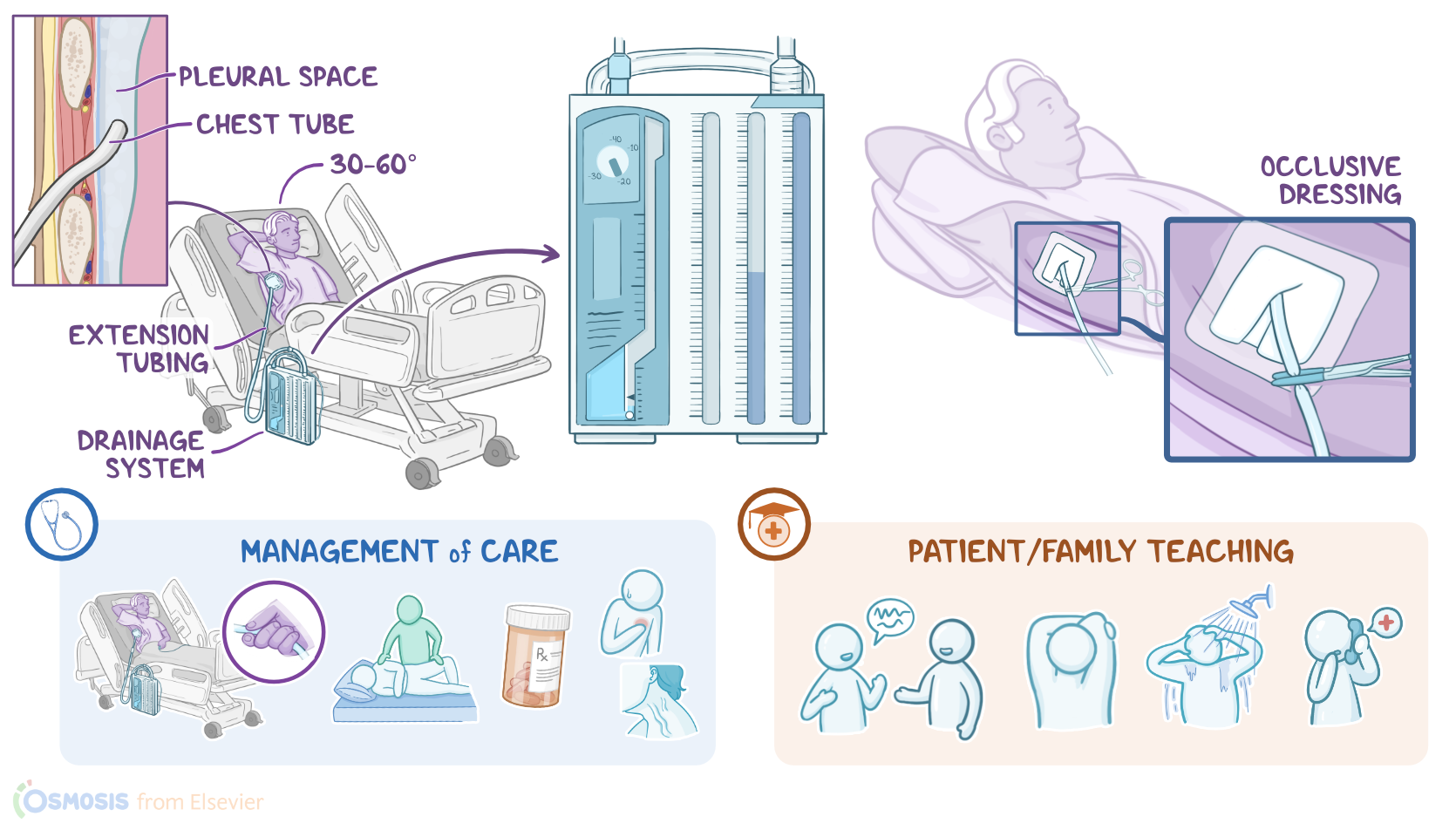
A chest tube can be used to remove air, fluids, or blood from the pleural space; to prevent air or fluid from reentering the pleural space; and to reestablish intrapleural and intrapulmonary pressures after surgery or trauma, in order to re-expand the lungs. A chest tube can also be inserted into the mediastinum after open heart surgery to drain fluid from the pericardial sac. Now, let’s quickly review the physiology of the pleura, which is a two-layered serous membrane that covers the lungs. The first layer of the pleura adheres to the surface of the lungs, called visceral pleura, whereas the second layer lines the chest wall, and it’s called the parietal pleura. Between these two layers there’s the pleural space, which is typically filled with a small amount of serous fluid that prevents friction between the two layers while breathing.
Moreover, let’s look at the physiology of breathing, which consists of two stages: inspiration and expiration. Inspiration is an active process, meaning that it requires muscles such as the diaphragm and the intercostal muscles to contract, which increases the intrathoracic volume and lowers the intrapulmonary pressure below the atmospheric pressure. This pressure gradient makes air flow from a high pressure area, meaning the atmospheric air, to a lower pressure area; so air is pulled inside the lungs. On the other hand, expiration is a passive process, meaning that it doesn’t require muscle contraction. That’s because the lungs have a special feature called elastic recoil, meaning they have a tendency to return to their normal size after being expanded. This allows the lungs to deflate after inspiration, decreasing the intrathoracic volume and increasing the intrathoracic pressure.
This process passively pushes the air from the area of higher pressure, which is the lungs, to the area of lower pressure, which is the atmosphere.Now, one end of the chest tube is typically inserted through the rib cage into the pleural space, while the other end is connected to extension tubing that drains into a drainage system. The most commonly used drainage system is the three-compartment drainage system. This system consists of three interconnected chambers: First, the collection chamber connects directly to the chest tube, and it collects air and fluid from the pleural cavity. Fluid stays in this chamber, while air flows to the next chamber, called the water seal chamber. This chamber acts as a one-way valve that allows air to flow into it during exhalation, and prevents air from moving back into the pleural space during inhalation. It is kept filled with 2 cm of sterile water that rises and falls during inhalation and exhalation, a process called tidaling.
When tidaling is present, we can be sure the chest tube is present. The suction control chamber is used to regulate the prescribed amount of suction, and it can be dry or wet. In wet suction devices, the amount of suction is regulated by the level of sterile water in the chamber, which is typically at -20 cm of pressure. In dry suction devices, a mechanical regulator is used to adjust the suction level. Other types of drainage systems include digital drainage systems, as well as a drainage system called the Hemlich chest drain. It is used to remove air from the pleural space in cases of a small pneumothorax where drainage or suction are not needed. It consists of a one-way flutter valve contained within a plastic tube. This device has an inlet nozzle, which allows air to pass from the pleural space to the valve; and an outlet nozzle, which allows air to flow to the outside.
All right, now the indications of chest tube placement include air in the pleural space, or pneumothorax, blood in the pleural space, called a hemothorax, or serous fluid from the pleural space, called a hydrothorax. Now, placing a chest tube can be done in the emergency room, the operating room, or at the bedside, and a couple of measures should be taken before inserting it. First is to make sure that the client is aware of the procedure and to obtain informed consent. Next is to perform an X-ray to confirm the affected side of the chest. Finally, gather the equipment needed for the procedure. Now, once everything is set up, the procedure begins by placing the client on the healthy side of the chest, with the arm on the affected side raised above the head to expose the midaxillary line.
The client’s head should also be elevated 30 to 60 degrees to minimize the risk of injury to the diaphragm. To insert the chest tube, first an antiseptic solution is used to cleanse the point of chest tube entry, which varies depending on the procedure. For draining fluid from the pleural space, the needle is typically inserted between the fifth or sixth intercostal space. On the other hand, when draining air, the needle is inserted between the second and third intercostal space, because air tends to pool at the top of the lungs. Now, after cleansing the point of entry, remember that the incision is made over the top of the inferior rib to avoid injury to intercostal blood vessels and nerves, which lie behind and below each rib. Next, a clamped chest tube is inserted into the incision and sutured into place; and the insertion site is covered with an occlusive dressing to prevent air from entering the pleural cavity.
Finally, the tube placement should be confirmed with an X-ray. Okay, let’s look at the nursing care you’ll provide to a client with a wet-suction chest tube. Your priority goals of care are to assist with chest tube insertion, promote lung expansion, and monitor for complications. Now, you can assist with the chest tube insertion by confirming informed consent has been obtained and premedicating your client with the prescribed analgesic. Set up the CDU by filling the water seal chamber with sterile water to the 2 cm mark and then filling the suction control chamber with sterile water to the -20 cm level. After the CDU is ready, assist with positioning your client for the procedure and providing reassurance during the insertion of the chest tube. Once the chest tube is in place, connect the drainage tube to the chest tube, and remove the clamp. Secure all of the connections with occlusive tape to prevent air leaks or disconnections.
Then, connect the suction control chamber to the suction unit, and increase the pressure until you see gentle, steady bubbling in the chamber. Assist your client into a semi-Fowler position and institute pulse oximetry so their oxygen saturation can be monitored. Lastly, place two soft-tipped hemostats by the bedside so they can be retrieved quickly. To promote lung expansion, ensure the CDU is functioning properly. Begin by ensuring the CDU is kept in an upright position and at a level lower than the client’s chest. Be sure to watch the water level in the water seal chamber, because it can evaporate over time; refill it if the water level drops below the 2 cm water mark. Likewise, because the continuous bubbling in the suction control chamber promotes evaporation, check this chamber often and keep the water in this chamber filled to the prescribed level.