Child maltreatment: Nursing
Child maltreatment refers to physical, sexual, or psychological abuse or neglect committed by another individual such as a parent or other caregiver. Abuse refers to any act that causes harm or significant risk of harm to a child; whereas neglect is the failure to provide the basic needs of a child.
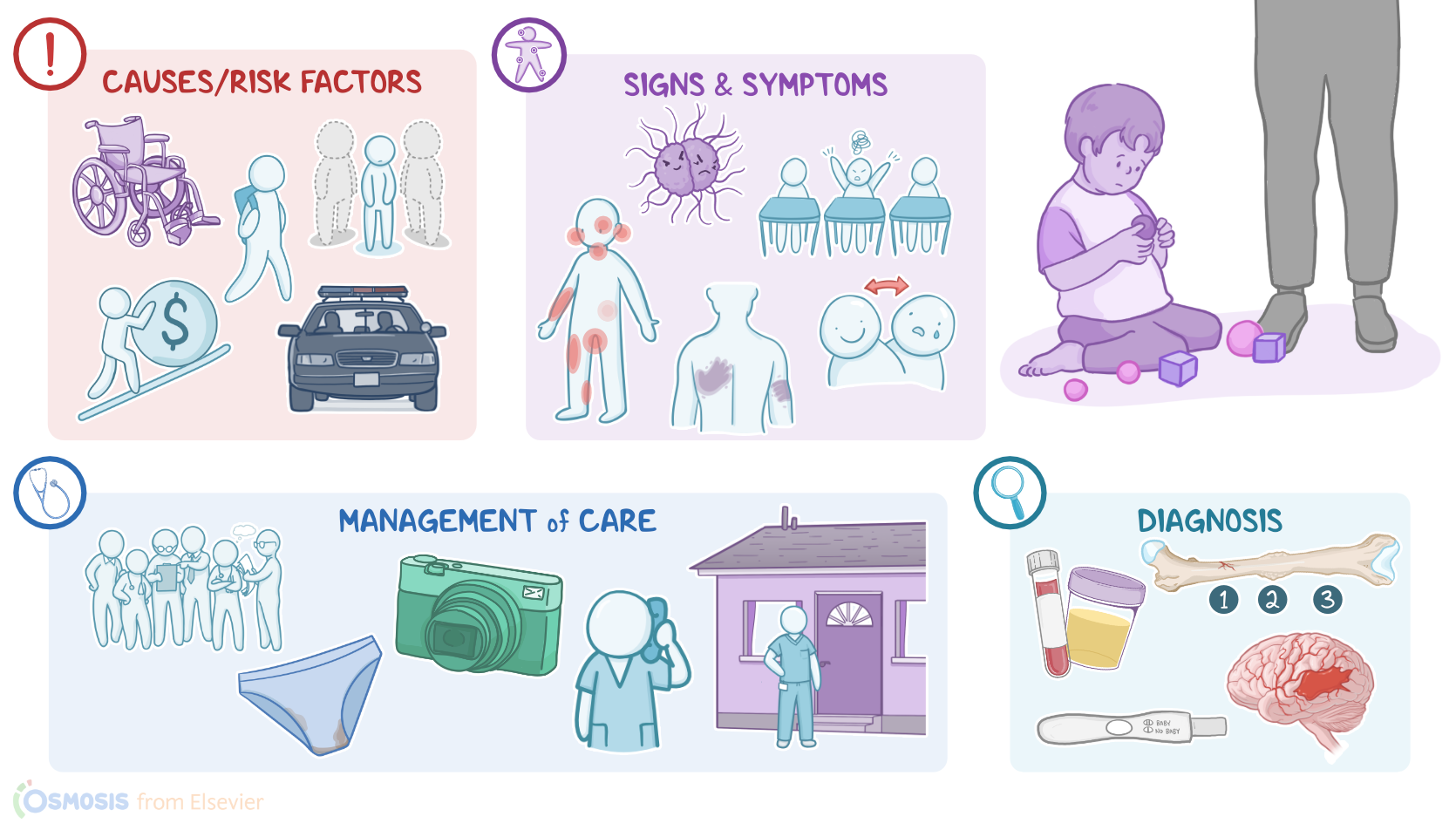
Now, risk factors for child maltreatment can be related to the child or the abuser. Factors related to the child include prematurity, and the presence of physical, psychological, or cognitive disabilities. Child maltreatment is also more common in children of younger age, if the child has behavioral problems, or if the child is unplanned or unwanted.
Now, regarding the factors related to the caregiver, important risk factors include low self-esteem, poor impulse control, young age, low educational achievement, poor social support, mental illness, such as depression, anxiety and substance misuse, or and when there is a biologically unrelated adult male living in the household.
Social factors that increase the risk of child maltreatment include stressful situations such as poverty, unemployment, eviction, or involvement with law enforcement. In addition, parents or caregivers who have experienced child abuse or domestic violence are more likely to be abusive.
Alright, now, there are several types of child maltreatment, including physical, emotional or psychological, sexual, and medical maltreatment. First, physical refers to any intentional physical injury that can result in injuries such as fractures, burns, bites, internal bleeding, or even death. In infants, a particular manifestation of physical abuse is shaken baby syndrome, where violent shaking of a baby is so traumatic that it causes subdural hemorrhage; that can lead to cerebral edema and death. Physical neglect is the failure to provide a child with food, shelter, and supervision. Physical neglect can also be manifested in abandonment, where the child is left alone, and the location of the parents or caregivers is unknown.
There’s also emotional or psychological abuse, which involves saying or doing things that undermine a child’s emotional development or self-esteem, resulting in the child feeling worthless, unloved or unwanted. This type of abuse can include threats, criticisms, rejection, or public shaming. Emotional and psychological neglect is when the emotional needs are not met, or if the child is exposed to domestic violence.
Next, sexual abuse includes any form of sexual contact or exploitation of a child. These are usually acts to provide sexual gratification of an adult and include but are not limited to touching, watching sexual acts, involving the minor in oral or penetrative sex, as well as sexual exploitation or trafficking,
Finally, medical abuse is mostly represented by fabricated or induced illness, formerly known as Munchausen syndrome by proxy. This is a rare form of child abuse where the carer fakes an illness in a child by seeking medical attention for fabricated symptoms, such as apnea, gastrointestinal disturbances, or seizures, resulting in unnecessary and excessive medical care.
Now, child maltreatment may present with different clinical manifestations depending on the type of the abuse or neglect. For instance, children experiencing physical abuse may present with bruises, and often, especially multicolored bruises, which indicates multiple assaults that are in different stages of healing. The areas of bruises that should raise supicion of child abuse are the soft parts of the body, like the cheeks and eyes, ears, neck, buttocks, flexor surfaces, or around the genitals, which are not commonly affected by unintentional injuries.
Another common finding includes unusual patterns of injury, like belt and rope marks, hand marks, and bite marks.
When it comes to burns, these are usually induced by a child being forcibly submersed into hot water. Signs of this include areas of the body that have been left unburned, like creases in the abdomen and parts of the palms and soles of the feet, reflecting a crouched, curled up position of the child. Likewise, the area from which the child was held will also be spared and show a prominent edge. Round, punctate burns may also be caused by cigarettes.
Finally, abused children may present with fractures, including rib fractures, especially posteromedial ribs that may be caused from squeezing a child too hard, spiral midshaft fractures of the humerus caused by traction or twisting the arm, and fractures of the hands or feet in children who haven’t started walking yet.
Now, maltreatment that is not physical is much more difficult to identify as the clinical manifestations are not always apparent. However, children experiencing emotional abuse or neglect may present with fear of the caregiver, rarely touching or looking at them and crying when it’s time to go home. They might also distrust other adults, like physicians and the nurses, or may have fear of the dark.
These children also commonly have mood disorders, anxiety, speech and learning disorders, or delayed physical and mental development. They also commonly have disruptive behavior at school, poor social skills, substance misuse, and a tendency to self-harm.
In sexual abuse, the child may have torn or stained underwear, difficulty walking or sitting, as well as bruises, swelling or itching on external genitalia, anal region, or the oropharynx. They might also present with urinary tract infections or sexually transmitted infections, while another clue might be having advanced knowledge about sexual acts compared to individuals of the same age.
| CHILD MALTREATMENT | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| CAUSES AND RISK FACTORS |
| |
| PATHOPHYSIOLOGY |
| |
| SIGNS AND SYMPTOMS |
| |
| DIAGNOSIS |
| |
| TREATMENT |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
No notes for this video yet
Try adding a note below