Complete metabolic panel (CMP) - Chloride: Nursing
Complete metabolic panel (CMP) - Chloride: Nursing
MidTerm
MidTerm
Notes
| CHLORIDE | ||
| KEY POINTS | NOTES | |
| PHYSIOLOGY |
| |
| PATHOLOGY |
| |
| INDICATIONS |
| |
| NURSING IMPLICATIONS |
| |
Transcript
A client arrives at the emergency department by ambulance with a report of fatigue and weakness after recurrent episodes of vomiting over the past few days. Based on these findings, a basic metabolic panel, or BMP is ordered to check the client’s electrolytes, including their chloride level.
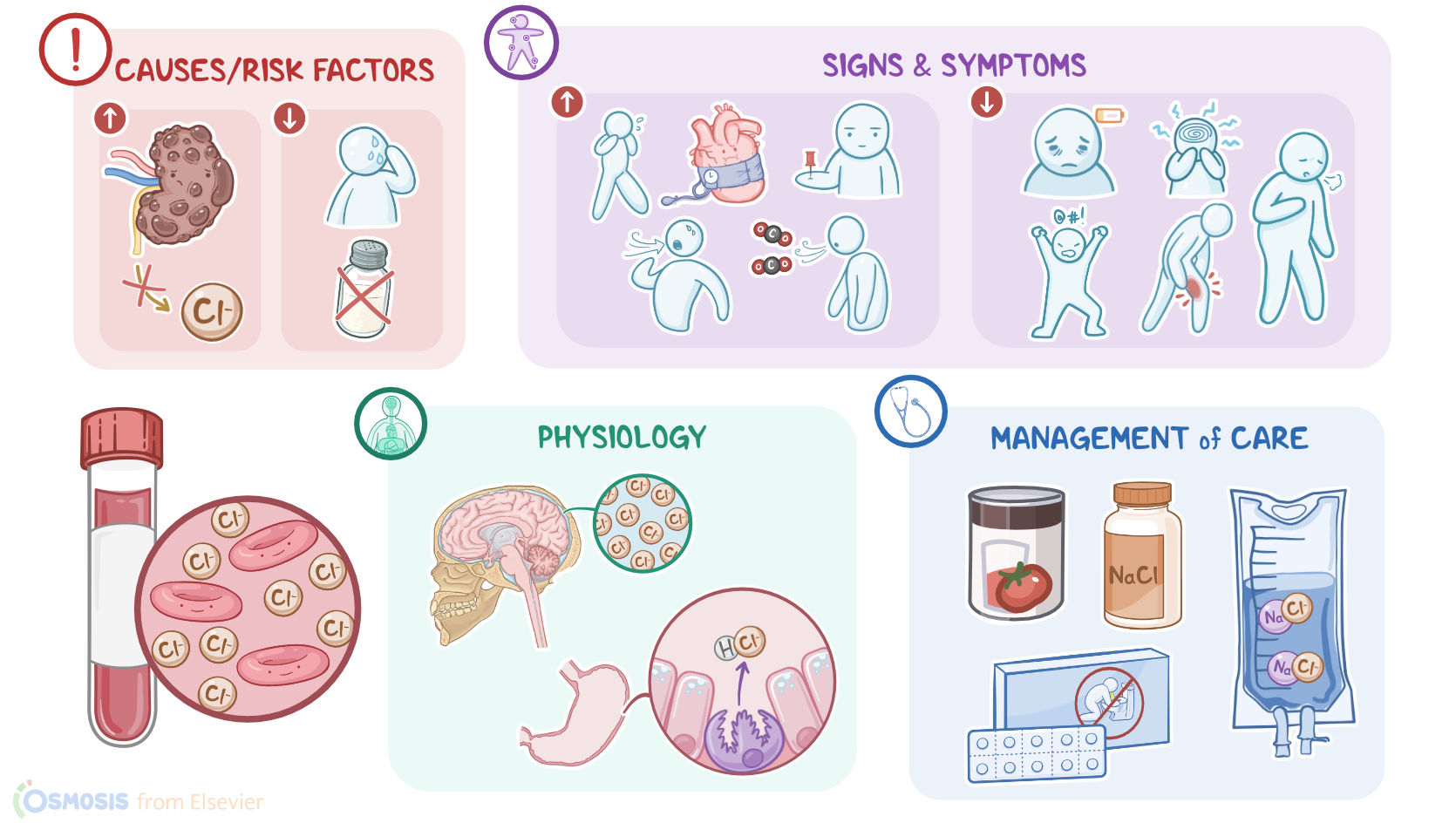
Now, chloride, abbreviated as Cl-, is a negatively charged ion, or anion. Most of the body’s chloride is found in the extracellular fluid, and it is often found associated with positively charged ions, like sodium and potassium. Chloride helps to maintain fluid balance, serum osmolality, and acid-base balance. There’s a significant amount of chloride in the cerebrospinal fluid, and it’s secreted by the gastric parietal cells in the form of hydrochloric acid to promote digestion.
Chloride mostly comes from the diet where it can be found in a variety of foods that are also high in sodium, such as processed meat, canned fish and vegetables, as well as table salt. Once ingested, a small amount is eliminated through the gastrointestinal tract, while most of it is excreted through the kidneys in the urine.
Now, plasma levels of chloride can be measured on its own, or as part of a CMP, or a complete metabolic panel; which is also called a basic metabolic panel, or BMP. In adults, normal chloride values range from 96 mEq/L to 106 mEq/L.
Alright, there are certain conditions that can cause a high serum chloride level, or hyperchloremia. Hyperchloremia often happens along with hypernatremia, or a high sodium level; so, when the sodium level rises, so does the chloride level. On the other hand, chloride has an inverse relationship with bicarbonate, so a decrease in bicarbonate, like with acidosis, is associated with an increase in chloride. In fact, hyperchloremic acidosis can be the result of severe diarrhea, where excessive amounts of sodium bicarbonate is excreted in the stools.
Hyperchloremia can also be caused by decreased excretion by the kidneys, like with renal failure; or with high levels of aldosterone, a hormone secreted by the adrenal glands that causes retention of sodium and chloride. Finally, hyperchloremia can be caused by an excessive intake of sodium chloride from the diet or saline infusions.
Now, when the chloride level gets too high, clinical manifestations will mirror the underlying cause. So, if hyperchloremia is associated with hypernatremia, then edema, hypertension, tachycardia, tachypnea, and dyspnea can be present. In cases of metabolic acidosis, common manifestations include a decreased level of consciousness and Kussmaul respirations, as the body attempts to restore a normal pH by blowing off excess carbon dioxide.
At the other end of the spectrum is hypochloremia, which is when the level of chloride in the serum is too low. Now, hypochloremia often happens along with hyponatremia, or a low sodium level; so, when the sodium level rises, so does the chloride level. On the other hand, chloride has an inverse relationship with bicarbonate, so an increase in bicarbonate, like with alkalosis, is associated with a decrease in chloride. In fact, hypochloremic alkalosis can be the result of severe vomiting or prolonged nasogastric suctioning, where excessive amounts of hydrochloric acid is lost from the stomach.
Other causes of chloride loss include excessive diaphoresis, as well as cystic fibrosis, a genetic disease characterized by blocked chloride transport in cell membranes and chloride loss in the sweat. Lastly, hypochloremia can be caused by decreased intake, like with salt-restricted diets.
Alright, when the chloride level gets too low, clinical manifestations will mirror the underlying cause. So, if hypochloremia is associated with hyponatremia, lethargy, altered mental status, and irritability can be present, as well as manifestations of neuromuscular irritability, like muscle twitching or cramping. In cases of metabolic alkalosis, common manifestations include slow and shallow respirations, as the body attempts to restore a normal pH by retaining carbon dioxide.
Now, a client’s chloride level is typically measured along with other electrolytes when they are experiencing a condition that can lead to electrolyte imbalance. Chloride will also be measured when there are signs or symptoms of high or low serum chloride.