Congenital diaphragmatic hernia: Nursing
Congenital diaphragmatic hernia: Nursing
Acute Final
Acute Final
Notes
| CONGENITAL DIAPHRAGMATIC HERNIA | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
| CAUSES AND RISK FACTORS |
| |
| PATHOPHYSIOLOGY |
| |
| SIGNS AND SYMPTOMS |
| |
| DIAGNOSIS |
| |
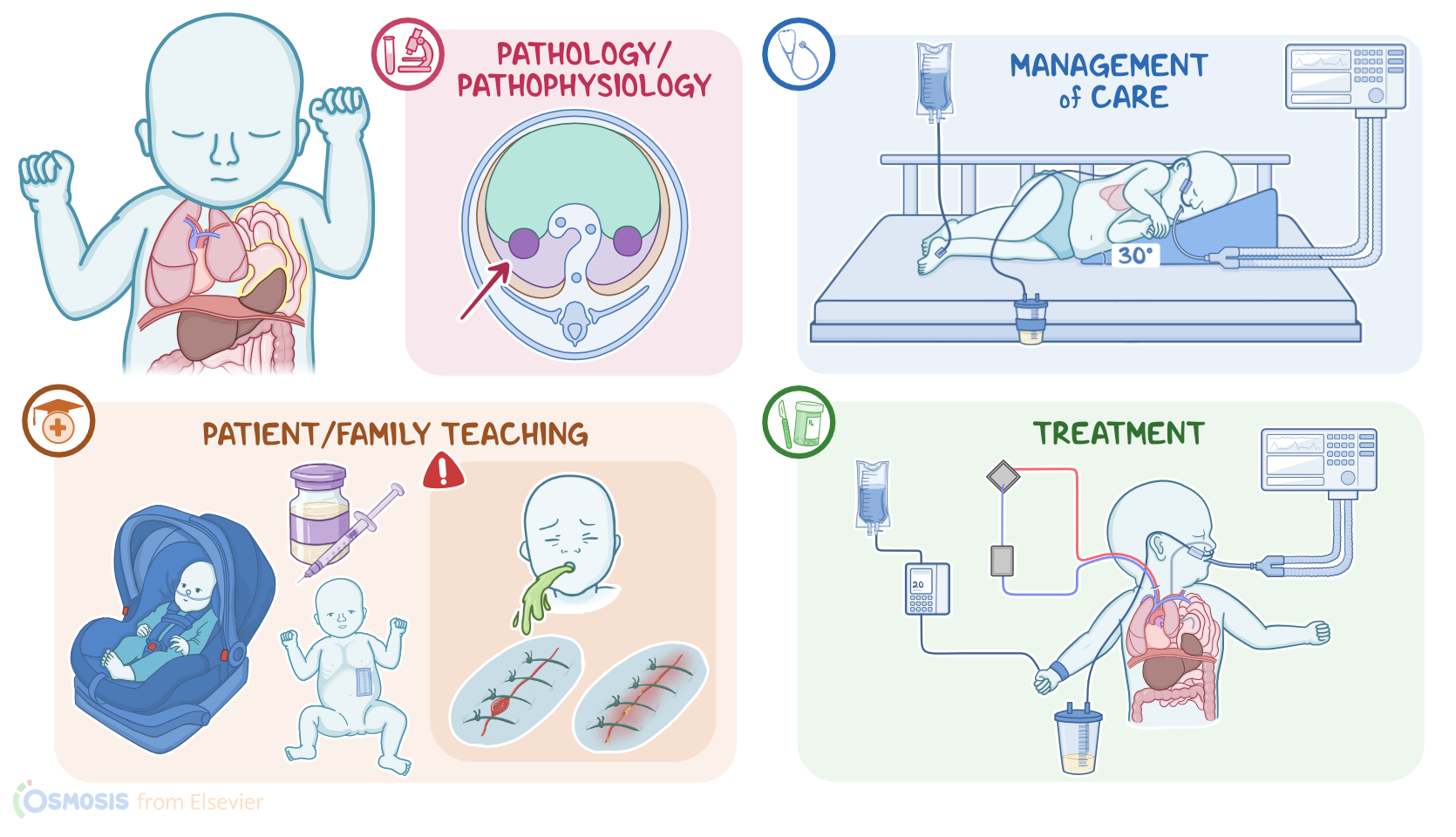
| TREATMENT |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
Transcript
Content Reviewers
Congenital diaphragmatic hernia is a development defect of the diaphragm in which an opening in the diaphragm allows the abdominal organs to herniate into the thorax. Herniation can develop on any or both sides of the diaphragm but it typically occurs at the left side of the diaphragm.
Alright, let’s start by reviewing the anatomy and physiology of the diaphragm. During intrauterine life, the diaphragm develops by the midline fusion of the paired retroperitoneal folds.
This results in the formation of a dome-shaped sheet of skeletal muscle that divides the thoracic cavity from the abdominal cavity.
Now, the diaphragm is the chief muscle for inspiration. When it contracts, the diaphragm moves downwards, which increases the volume of the thoracic cavity, and with it,the volume in the lungs. This makes the intrapulmonary pressure fall below the atmospheric pressure, creating a partial vacuum that allows fresh air to be sucked in.
Now, the exact cause of congenital diaphragmatic hernia is unknown, but it's believed to be associated with certain genetic risk factors that can interfere with the development of the diaphragm, including chromosomal abnormalities like the trisomy 13, 18, or 21.
Alright, the pathology of congenital diaphragmatic hernia starts during the fetal period. If during development, retroperitoneal folds don’t fuse properly, the newly formed diaphragm will have a hole in it. This allows abdominal organs, like the stomach and intestines, to herniate into the thoracic cavity.
The herniated organs push against the lung on the affected side, preventing the lungs from growing to normal size, a condition called pulmonary hypoplasia.
Pulmonary hypertension develops along with a right-to-left shunting through the ductus arteriosus and foramen ovale, resulting in deoxygenated blood being pumped to the body, resulting in systemic hypoxemia.
Long-term complications of congenital diaphragmatic hernia include chronic lung disease, gastroesophageal reflux disease, or GERD for short, and developmental delay, as well as a recurrence of the diaphragmatic hernia.
Congenital diaphragmatic hernia typically presents with signs of respiratory distress and cyanosis. Upon physical assessment, there is typically a barrel-shaped chest and a scaphoid-shaped abdomen. Respiratory distress can worsen with bag mask ventilation as the bowel distends with air and further compromises lung function.
Inspection of the thorax shows asymmetrical chest expansion. During auscultation, breath sounds are reduced or absent on the affected side, and bowel sounds can be heard in the chest. In addition, in a left-sided congenital diaphragmatic hernia, the heart tones are also displaced from their normal point of maximal intensity, due to the shift of the mediastinum.
The diagnosis of congenital diaphragmatic hernia is often made before birth during routine obstetric ultrasound examination.
If the defect is not detected prenatally, the diagnosis can be suspected at birth based on the clinical presentation.
A chest X-ray will show abdominal contents herniating into the thoracic cavity, in addition to pulmonary hypoplasia and displacement of the mediastinum.
The initial treatment of diaphragmatic hernia aims at stabilizing pulmonary and cardiovascular function. This can be done with endotracheal intubation, ventilatory support, and fluid administration, along with the insertion of a nasogastric tube to decompress bowel contents. Intubation and mechanical ventilation is required, and in some cases, extracorporeal membrane oxygenation, or ECMO, might be needed.
Definitive treatment consists of surgical repair, during which the herniated abdominal structures are pushed back to the abdominal cavity and the diaphragm opening is stitched shut. After the procedure, a chest tube is often placed into the thoracic cavity to drain fluids or air, which helps to inflate the lungs.
Alright, let’s talk about the care you’ll provide for a newborn diagnosed with a congenital diaphragmatic hernia. Your priority goals are to support pulmonary and hemodynamic function and provide emotional support.