Cryptorchidism: Nursing
Cryptorchidism: Nursing
Watch later
Watch later
Notes
| CRYPTORCHIDISM | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
| CAUSES AND RISK FACTORS |
| |
| PATHOPHYSIOLOGY |
| |
| SIGNS AND SYMPTOMS |
| |
| DIAGNOSIS |
| |
| TREATMENT |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
Transcript
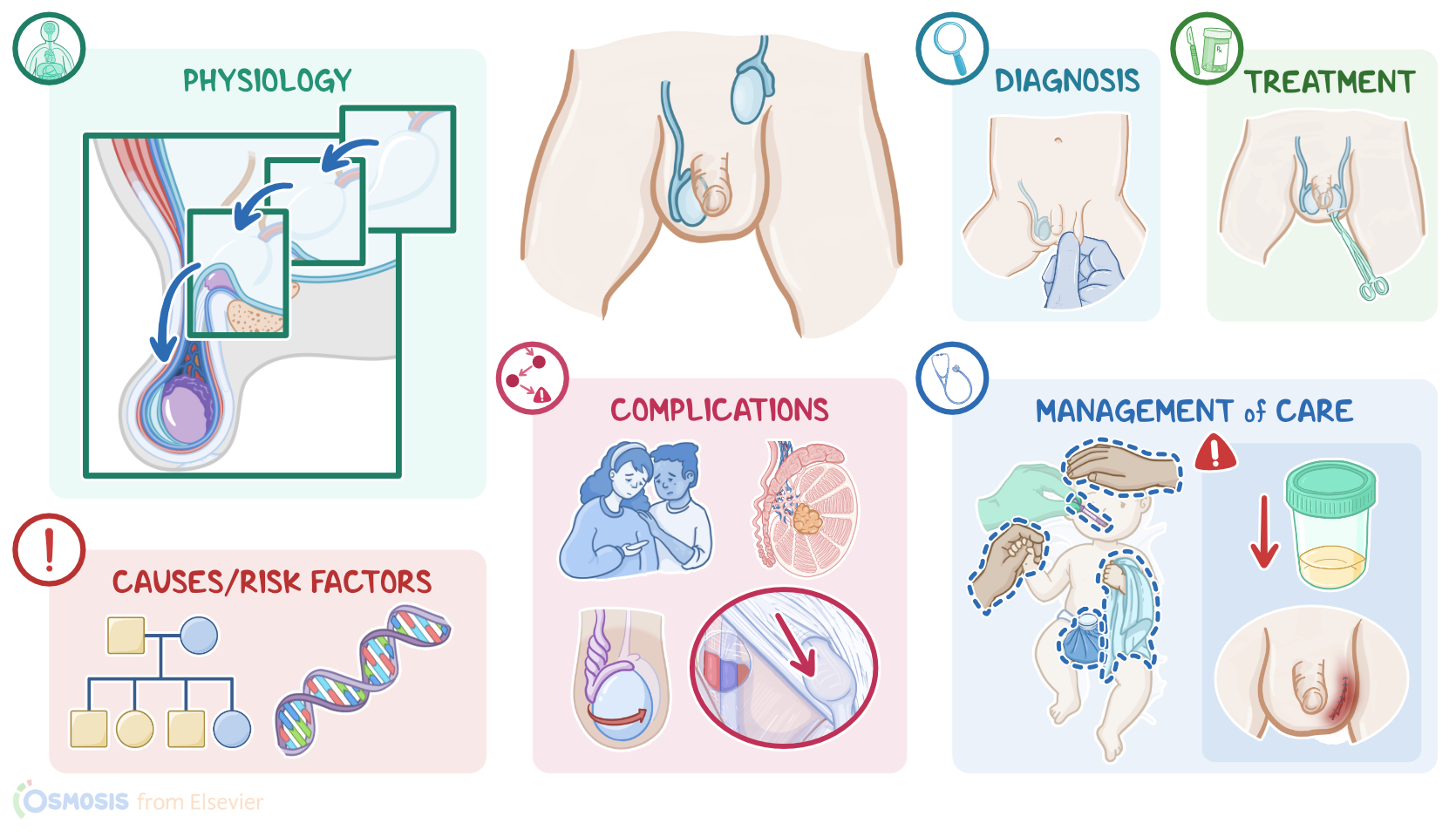
Cryptorchidism, also known as undescended testis, is a condition characterized by partial or abnormal descent of one or both testicles into their normal position within the scrotal sac. Cryptorchidism is commonly seen in neonates, and, in most cases, it spontaneously resolves during the first year of life.
First, let’s cover some basic physiology of testicular descent. Initially, during intrauterine development, testes develop in the abdomen.Here, each testicle is anchored to the labioscrotal swelling, which is the future scrotum, by a fibrous cord called the gubernaculum
Between the 7th and 12th week of fetal development, the gubernaculum shortens, eventually pulling the testicles down toward the inguinal canal, where they usually stay until the 7th month of intrauterine development. Finally, during the last month of pregnancy,the testes descend into the scrotum. The process is controlled by an androgen hormone called testosterone. Once in the scrotum, the testes have an adequate environment for normal sperm production, also known as spermatogenesis, which starts at puberty.
Finally, during fetal development, a small cremasteric muscle develops within the gubernaculum. The main function of this muscle is to retract the testicle toward the inguinal canal when the outside environment is not suitable for testes, like, for example, when it’s too cold.
Now, the exact cause of cryptorchidism remains unknown. Some theories suggest that cryptorchidism may occur due to gubernaculum abnormalities, while others connect this condition with androgen deficiency. Cerebral palsy and conditions associated with abdominal wall defects, like Prune-Belly syndrome, can also result in cryptorchidism. Important risk factors for cryptorchidism include family history, as well as birth-related risk factors, such as preterm birth; and low birth weight.
Additionally, clients with some congenital conditions have a higher incidence of cryptorchidism than others. These include meningomyelocele, which occurs when the spinal cord and the surrounding meninges protrude through an opening in the vertebrae into a cyst-like pouch; hypospadias, which is a condition characterized by the opening of the urethra along the underside of the penis; and congenital malformation syndromes, like Noonan, Down, and Prader-Willi syndromes. Finally, maternal conditions, like diabetes and obesity, as well as maternal lifestyle factors, like smoking, and alcohol consumption during pregnancy, can increase the risk of cryptorchidism.
Now, let’s switch gears and move on to pathology. Gubernaculum abnormalities can affect testicular descent from the abdomen to the inguinal canal. On the flip side, in androgen deficiency, there’s not enough testosterone, to complete testicular descent from the inguinal canal, to the scrotum. Next, in clients with cerebral palsy, there might be spasticity of the cremaster muscle, which can cause the retraction of the testicle from the scrotal sac into the inguinal canal. Finally, abnormalities of the abdominal wall can mechanically obstruct the testicular path to the scrotal sac and block the testicular descent.
Cryptorchidism can cause serious complications, including testicular torsion, infertility, inguinal hernias, and even testicular cancers, such as seminoma. There are also psychological complications, including embarrassment, shame, and depression, which can have a strong impact on the client’s self-esteem.
The main clinical manifestation of cryptorchidism is the absence of one or both testes in the scrotal sac, which usually results in the asymmetry of the scrotal sac. Diagnosis of cryptorchidism is based on the client's history, and physical assessment, which includes palpation of the scrotal sac. This reveals the absence of one or both testes. In most clients, the undescended testicle can be palpated within the inguinal canal, but in some cases, the testicle can be located within the abdominal cavity. In this case, laparoscopy or open surgery can be used to directly visualize the testicle within the abdominal cavity.
Now, it’s important not to confuse cryptorchidism with a retractile testicle. In this condition, the testicle lies within the inguinal canal, from where it can be easily pushed back into the scrotal sac. The testicle remains in the scrotal sac until it decides to retract and go back into the inguinal canal.
Now, treatment-wise, it’s worth mentioning that watchful waiting can be indicated for 6 months after diagnosis, in clients younger than 18 months. That’s because during this time, the testicle can descend on its own.
However, beyond that time frame, treatment is indicated through orchidopexy, which means surgical repositioning of the affected testicle into the scrotal sac, where it’s permanently fixated. Orchidopexy is usually done before two years of age in clients in whom the testicle failed to descend spontaneously. On the flip side, clients with a retractile testicle do not require treatment, because this condition usually resolves on its own during puberty.
Alright, let’s look at the nursing care you’ll be providing for a child with cryptorchidism. Your priority nursing goals are to manage postoperative pain and monitor for postoperative complications.
To manage postoperative pain, start by assessing the child for signs of pain by checking for behaviors such as crying, restlessness, irritability, muscle tension, and their ability to be consoled. Then, administer the prescribed analgesic medication and institute comfort measures such as encouraging caregiver presence; allowing them to have a favorite toy or blanket; reducing environmental stressors; and applying cool packs to the surgical site.