Cushing syndrome and Cushing disease: Nursing
Notes
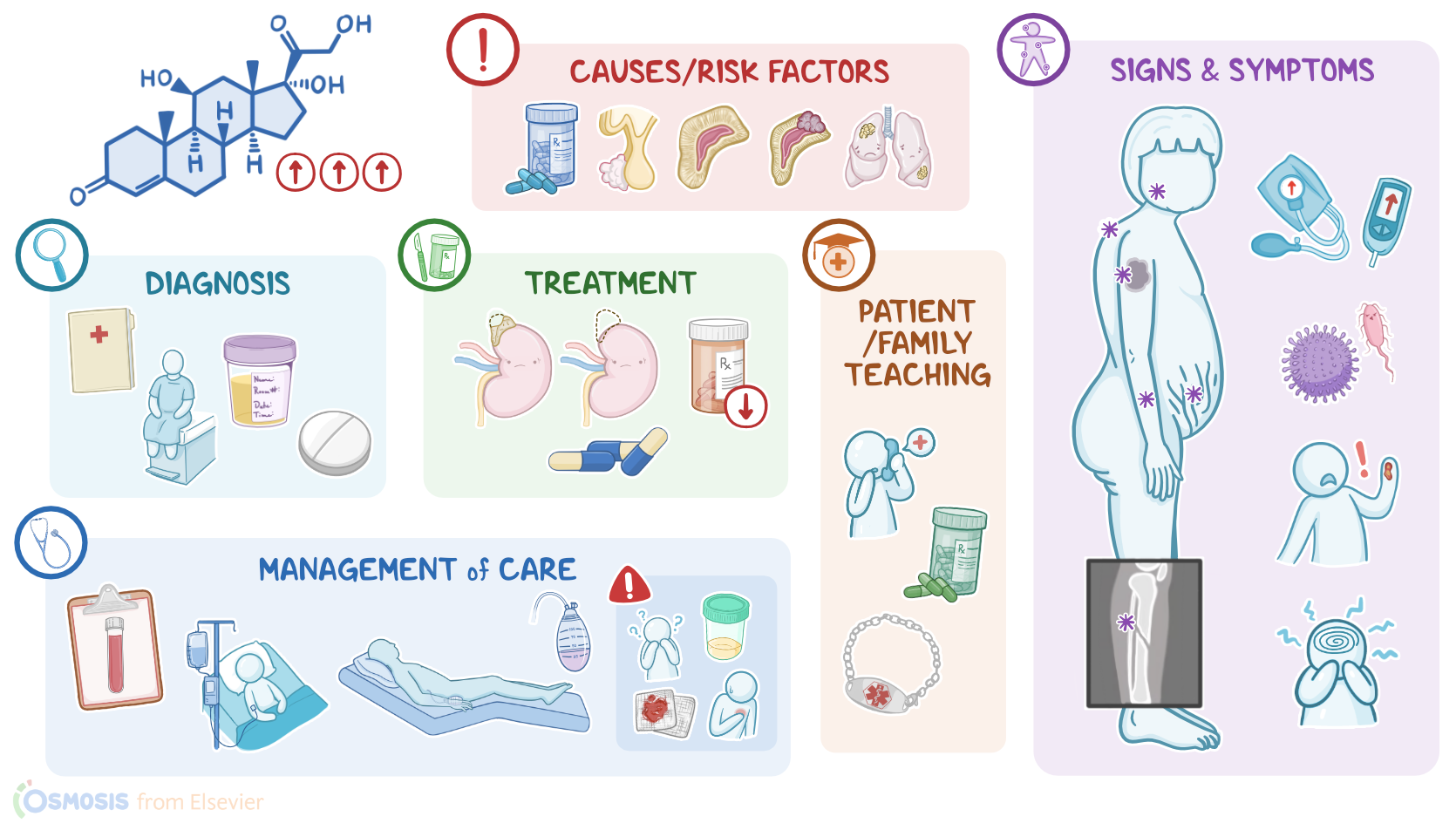
| CUSHING SYNDROME AND CUSHING DISEASE | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
| CAUSES AND RISK FACTORS |
| |
| PATHOPHYSIOLOGY |
| |
| SIGNS AND SYMPTOMS |
| |
| DIAGNOSIS |
| |
| TREATMENT |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
Transcript
Content Reviewers
Cushing syndrome is an endocrine disorder characterized by elevated cortisol levels in the blood. It can result from excessive production of cortisol from the adrenal cortex; or it can be iatrogenic, from the administration of glucocorticoid medications for a prolonged period of time. In some cases, elevated cortisol levels are secondary to an ACTH-secreting pituitary adenoma, which is called Cushing disease.
Now, let’s quickly review the anatomy and physiology of cortisol production. Normally, the hypothalamus, which is located at the base of the brain, secretes corticotropin-releasing hormone, known as CRH, which stimulates the pituitary gland to secrete adrenocorticotropic hormone, known as ACTH. ACTH then travels to the paired adrenal glands, one on top of each kidney, where it specifically targets cells in the adrenal cortex.
The adrenal cortex is the outer part of the adrenal gland and is subdivided into three layers: the zona glomerulosa, the zona fasciculata, and the zona reticularis. In the zona fasciculata, ACTH stimulates cortisol secretion. Cortisol is a glucocorticoid, and it’s involved in a number of things such as maintaining glucose levels, blood pressure, and the suppression of the inflammatory and immune response. Additionally, it can also influence things like mood and memory, as well as degrade collagen and connective tissue within the tissues.
Now, to make sure that these actions work for the benefit of the body, and not against it, free cortisol levels have to stay within the normal range. To do that, the body uses negative feedback, which means that high levels of cortisol make the hypothalamus and pituitary gland secrete less CRH and ACTH, respectively. This ultimately results in decreased stimulation of the zona fasciculata, so cortisol levels go down. Finally, bear in mind that cortisol secretion has a circadian rhythm, so cortisol levels are normally higher in the morning and at their lowest around midnight.
Okay, now, when it comes to what causes Cushing syndrome, the majority of cases occur in individuals using exogenous glucocorticoid medications, such as prednisone, over a long period of time. Alternatively, elevated cortisol levels can also result from increased endogenous production of cortisol. The most common reason for that is a pituitary adenoma, which is a benign tumor of the pituitary gland. When the pituitary adenoma secretes too much ACTH, that makes the zona fasciculata of both adrenal glands secrete excess cortisol, and this is known as Cushing disease. Other causes of endogenous Cushing syndrome are adrenal hyperplasia and tumors of the adrenal glands that make excess cortisol, like adrenal adenomas, which are benign tumors, and adrenal carcinomas, which are malignant tumors. Cushing syndrome can also be caused by ectopic ACTH production, which is when a tissue other than the pituitary gland secretes ACTH; most often, this occurs in clients with small cell lung cancer.
Now, the end result in Cushing syndrome is that cortisol levels are constantly higher than normal, so its effects are exaggerated. Excess cortisol leads to severe muscle, skin, bone breakdown which are the major protein stores of the body.
It can also impair glucose metabolism, causing elevated blood glucose and high insulin levels. Insulin, among its many actions, preferentially targets adipocytes or fat cells in the center of the body, around the waist and buttocks and the result is central obesity.
Moreover, high cortisol levels also cause hypertension, and the reason is twofold. Firstly, cortisol amplifies the effect of catecholamines on blood vessels. Secondly, excess cortisol can cross-react with mineralocorticoid receptors, which normally only bind related steroid hormones called mineralocorticoids, that are secreted by the zona glomerulosa of the adrenal cortex. Now, since glucocorticoids like cortisol and mineralocorticoids are chemically similar, the excessive cortisol can also bind to the mineralocorticoid receptor, and enact mineralocorticoid-like effects, such as fluid retention and increasing blood pressure.
Now, high levels of cortisol also inhibit the secretion of gonadotropin-releasing hormones from the hypothalamus, which control the normal function of the ovaries and testes. So cortisol excess can also impair gonadal function. In addition, excess cortisol dampens the inflammatory and immune response, making individuals more susceptible to infections. Finally, high levels of cortisol seem to impair normal brain function but the exact mechanism of that is unclear.
Regardless of the cause, the signs and symptoms of Cushing syndrome are directly related to the effects of excess cortisol on various target tissues. Typical manifestations include muscle wasting and thin extremities, skin thinning, easy bruising and abdominal striae or lines, as well as fractures due to osteoporosis or brittle bones. At the same time, there’s fat redistribution, so classic findings include a round, full moon shaped face, a buffalo hump, which is a fatty hump on the upper back, and truncal obesity, where fat gathers around the abdomen and trunk rather than in the limbs.
Finally, excess cortisol causes hyperglycemia or high blood glucose levels that can progress to diabetes mellitus; as well as hypertension and a high risk for cardiovascular disease. Other clinical findings include increased vulnerability to infections, poor wound healing, amenorrhea or absent menstrual bleeding and psychiatric or mental disturbances.
Diagnosis of Cushing syndrome starts with the client’s history and physical assessment, followed by measuring the free, or unbound cortisol in a 24-hour urine sample, in order to assess the total amount of cortisol excreted in the urine over a 24-hour period.
Alternatively, blood or saliva tests late at night can help check if there’s a normal cortisol circadian rhythm, which should rise in the morning and decrease at night.
Another option is also the low-dose dexamethasone suppression test, where the client is given a low dose of dexamethasone, which is an exogenous steroid that suppresses ACTH production in the pituitary gland. Normally, that causes a decrease in blood cortisol levels, but in clients with Cushing syndrome or Cushing disease, blood cortisol levels remain unchanged. If that test is positive, the next step is to determine the exact cause of endogenous cortisol production, so ACTH blood levels can be checked.
Low ACTH levels can be seen in adrenal adenomas and carcinomas, and that’s because of negative feedback. On the other hand, high ACTH levels can be seen in Cushing disease and ectopic ACTH production.
If ACTH levels are high, the next step is to perform a high-dose dexamethasone suppression test by injecting a high dose of dexamethasone. Unlike pituitary adenomas, ectopic ACTH production typically doesn't dampen even with high doses of dexamethasone, so blood cortisol remains high.
Finally, in some cases, the underlying cause can be confirmed with imaging studies. An MRI of the pituitary gland can show a pituitary adenoma, while a CT scan of the adrenals can give clues when adrenal pathology is suspected. Finally, a CT scan of the chest, abdomen, or pelvis can be done if an ectopic site of ACTH production is suspected.
Treatment of Cushing syndrome depends on the underlying cause. If it’s due to a tumor on one of the adrenal glands, then surgical resection of the adrenal tumor or the entire adrenal gland is the treatment of choice. If it’s due to exogenous medications, then the offending drug is gradually decreased and eventually stopped if possible.
It’s important to avoid sudden steroid withdrawal, though, because that can cause a potentially life threatening adrenal crisis. That’s because exogenous glucocorticoids inhibit ACTH production and, in turn, adrenal cortisol secretion, so the adrenal glands can be atrophied and may need months to recover fully. During that time, exogenous steroids, albeit in tapering doses, are needed for the body to function normally.