Developmental dysplasia of the hip: Nursing
Developmental dysplasia of the hip: Nursing
NUR243
NUR243
Notes
| DEVELOPMENTAL DYSPLASIA OF THE HIP | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
| CAUSES AND RISK FACTORS |
| |
| PATHOPHYSIOLOGY |
| |
| SIGNS AND SYMPTOMS |
| |
| DIAGNOSIS |
| |
| TREATMENT |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
Transcript
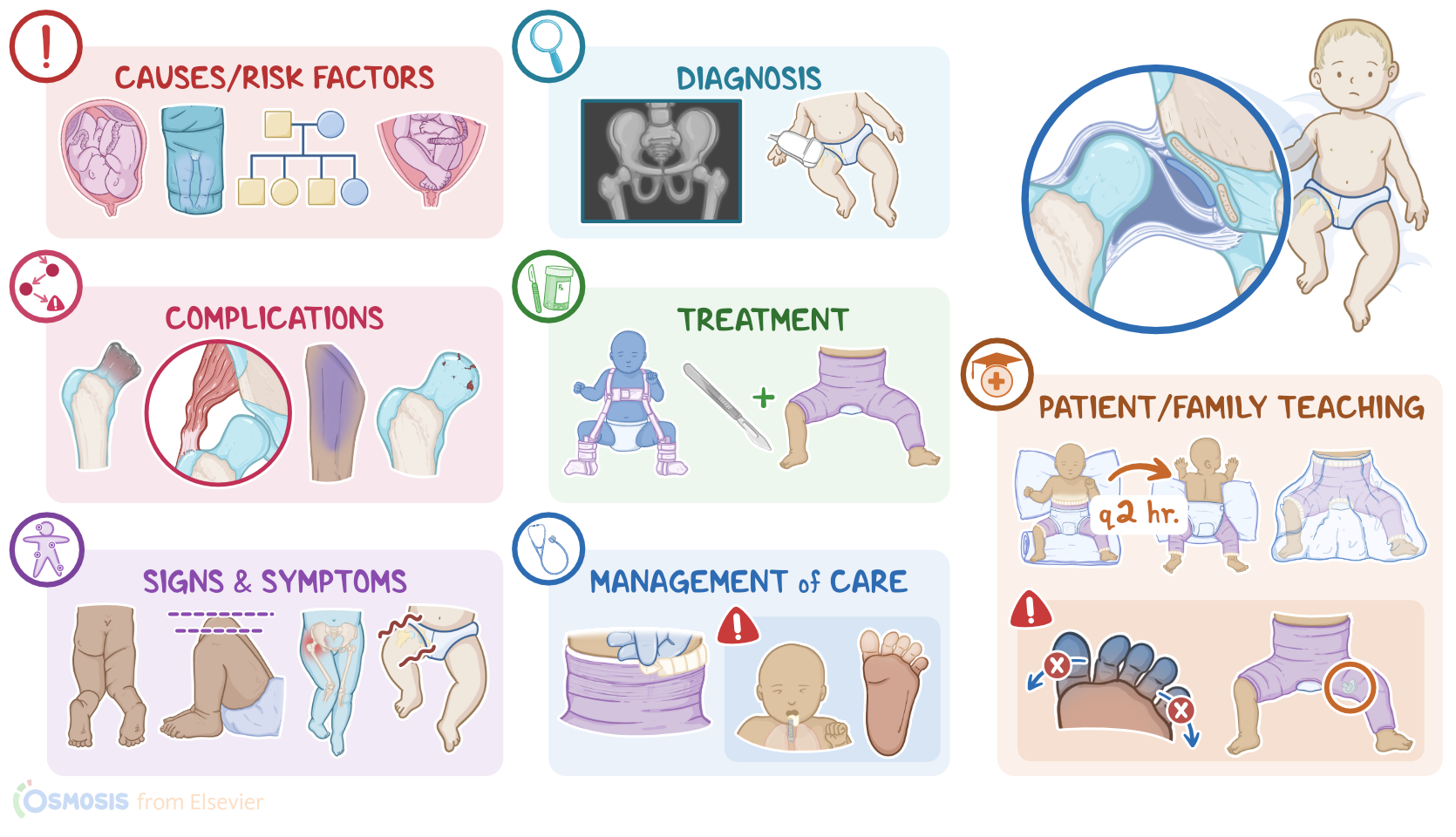
Developmental dysplasia of the hip is a condition where the socket or acetabulum and the femoral head are misaligned, resulting in an unstable hip joint. Typically, the condition is present at birth, but sometimes it appears later as the bones develop over time.Now, let’s go over some anatomy and physiology. The hip joint is also called the acetabulofemoral joint. The main function of the hip joint is to support the weight of the body while providing mobility. It is a ball and socket synovial joint, where the ball-shaped head of the femur sits and rotates within the acetabulum of the pelvis, which is a cup-shaped socket. At the bottom of the acetabulum, known as the acetabular fossa, arises a ligament called the ligamentum teres, that attaches to the fovea capitis, which is a depression found on the tip of the femoral head. This ligament helps with joint stability, especially during hip flexion and abduction.
Now, during embryonic development, the mesoderm is separated by a cleft to distinguish the acetabulum and the femoral head by the 7th week of pregnancy. The proper development of a hip joint requires that the femoral head stays fitted within the acetabulum, so that they both grow together keeping their sizes and shapes proportional. Finally, by the 11th week, the hip joint is fully recognizable. All right, now the exact causes of developmental dysplasia of the hip are unknown, but there are several risk factors. One of these is too much mechanical force being applied against a fetal thigh, which can cause the femoral head to slip out of the acetabulum. This can happen when a baby is lying in a breech position within the uterus. This sort of mechanical force can also occur with multiple gestations, macrosomic or large babies or with oligohydramnios, where there is not enough amniotic fluid to expand the uterine cavity.
Additionally, having congenital musculoskeletal deformities increases the risk for developmental dysplasia of the hip. Other risk factors include family history of developmental dysplasia of the hip joint, and being assigned female at birth. A final important risk factor is being improperly swaddled, so the infant’s legs are wrapped tightly in an extended position, instead of wrapped loosely so the legs can move freely.Developmental dysplasia begins during development, when the femoral head dislocates out of the acetabulum. As a result, they grow out of proportion to one another and are unable to form a stable joint. Moving on to pathology, the three main types of developmental dysplasia of the hip include dysplasia, where the head of the femur is in a shallow acetabulum, and it will dislocate on physical exam; subluxation, which is when the head of the femur is loose in the acetabulum, but it will not dislocate on physical exam; and dislocation, where there is no contact between the femoral head and acetabulum.
In addition, the acetabular structures will start hypertrophying within the acetabular fossa like the ligamentum teres and the transverse ligament. In other words, the socket becomes “more shallow”, making for a poor fit for the femoral head.In terms of complications, if the dislocation continues, the muscles around the hip will begin to atrophy. Less common complications include avascular necrosis of the femoral head, which results from reduced blood supply, femoral nerve palsy, and early osteoarthritis. Clinical manifestations of developmental dysplasia of the hip may differ according to the baby’s age. In neonates, the only sign might be laxity of the ligaments around the hip. An infant may present with a shortened leg on the affected side, as well as asymmetric gluteal or thigh skin folds. Ambulatory children often present with an abnormal gait or limp. The diagnosis of developmental dysplasia of the hip starts with the client's history and physical assessment. Babies up to 6 months of age are usually tested with the Barlow and Ortolani maneuvers.
The Barlow maneuver consists of adducting the hip while holding the knee straight, and when this pops the femoral head out of the socket, this raises suspicion of hip dysplasia. The Ortolani maneuver consists of flexing the baby’s hip at 90°, and then gently abducting it. If the femoral head was out of the socket, the Ortolani maneuver will cause it to slip back into the acetabulum, which will feel and sound like a clunk. After the age of 6 months, the hip abduction test can be used. The test begins with the hips flexed to 90° and then the thighs are gradually abducted. Normally the thighs can be abducted to 70° from the midline. In developmental dysplasia of the hip, abduction is under 45° because of muscle shortening in the affected hips. For older children, a Trendelenburg test can be performed, which is where the child is asked to stand on one leg for 30 seconds without leaning. A negative test is when the pelvis stays level, or rises, and positive when the pelvis drops toward the unsupported side. Finally, imaging tests can be used to confirm the diagnosis, by assessing the position of the femoral head and the structure of the acetabulum.