Erythema infectiosum (Fifth disease): Nursing
Erythema infectiosum (Fifth disease): Nursing
Watch later
Watch later
Notes
| ERYTHEMA INFECTIOSUM (FIFTH DISEASE) | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
| CAUSES AND RISK FACTORS |
| |
| PATHOPHYSIOLOGY |
| |
| SIGNS AND SYMPTOMS |
| |
| DIAGNOSIS |
| |
| TREATMENT |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
Transcript
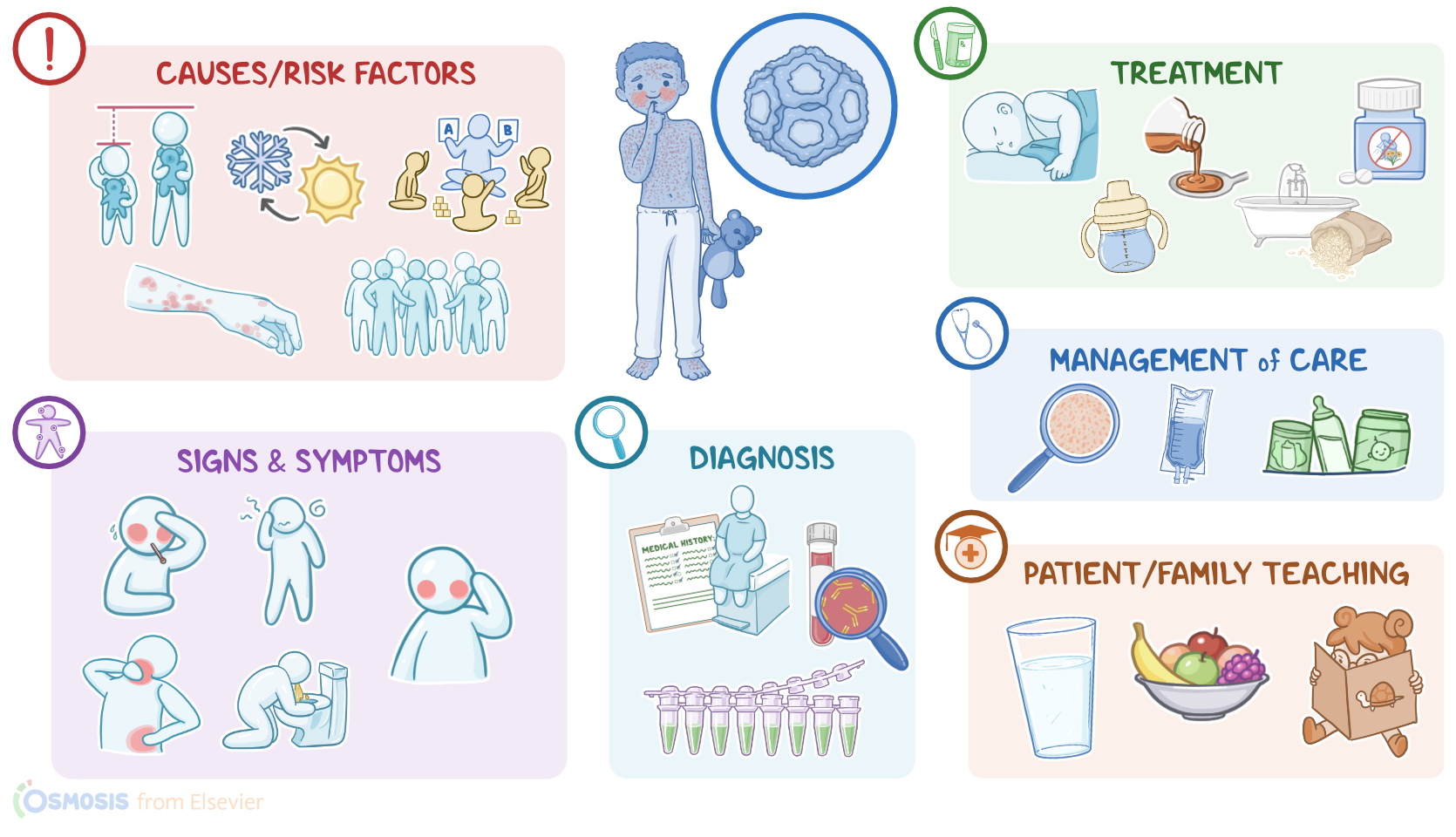
Erythema infectiosum, also known as fifth disease, is a common and highly contagious, self-limiting viral exanthem, or eruptive skin rash, caused by the human parvovirus B19. Erythema infectiosum is typically seen in children between the ages of five and fifteen years, and it’s characterized by a distinctive facial rash with a “slapped cheek” appearance.
Let’s start by discussing the physiology of the immune response. It all begins in the bone marrow, where undifferentiated hematopoietic stem cells begin to differentiate into different types of white blood cells. Some of these cells migrate to the thymus where they become mature T cells, also known as T lymphocytes, which defend us against intracellular viruses, fungi, and tumor cells. Additionally, they are responsible for long-term immunity.
Now, after a foreign antigen enters the body, it runs into antigen-presenting cells, like macrophages and dendritic cells, by whom it is engulfed and digested into fragments. These antigen fragments are then presented on their surface and recognized by T helper cells, which help activate B cells to produce antibodies against that antigen. Next, these antibodies bind to any affected cell that expresses the antigen on its surface, eventually enabling natural killer or NK cells and cytotoxic T cells to easily recognize and destroy them.
Now, the cause of erythema infectiosum is human parvovirus B19, which is a small DNA virus that belongs to the Erythroparvovirus genus and Parvoviridae family. Important risk factors for developing erythema infectiosum include age between five and fifteen years, late winter to early summer season, being in daycare, coming in contact with an infected individual, living in crowded living conditions, and immunodeficiency.
Okay, moving on to pathology. Human parvovirus B19 is primarily an airborne virus, meaning it most often spreads via small virus-containing droplets that get flung in the air when an infected client coughs or sneezes. If another person breathes in these droplets, or if they come in contact with infected surfaces and then touch their mouth, they can become infected.
Parvovirus B19 can also be transmitted through direct contact with respiratory secretions, and it is also considered a bloodborne virus, meaning it can be spread by exposure to infected blood and blood products.
Once the parvovirus enters the body, it binds to a specific receptor on the membrane of epithelial cells in the respiratory tract and enters the cell via endocytosis. Local macrophages and dendritic cells recognize the parvovirus and migrate to the lymph nodes, where they present the viral antigens to T helper lymphocytes, which then kick off an immune reaction. Meanwhile, instead of replicating in the epithelial cells, the parvovirus keeps traveling through cells and into the circulatory system until it reaches bone marrow, where red blood cells are made in a process called erythropoiesis.
Once there, the virus uses receptor-mediated endocytosis to enter erythroid progenitor cells, also called proerythroblasts, which are early cells that eventually become red blood cells. The virus uses these cells to replicate and mature, which is toxic to the cells and causes apoptosis, or cell death. This leads to erythropoiesis breakdown and fewer new red blood cells getting into the circulation. At the same time, when the cell dies, it bursts open, releasing copies of the virus into the blood, also called viremia. The immune system now starts producing specific immunoglobulin M, or IgM, and immunoglobulin G or IgG antibodies to fight the infection by forming immune complexes with the parvovirus B19 antigen.
Complications of the parvovirus B19 are rare in healthy clients, but in clients with underlying conditions, such as sickle cell anemia, hereditary spherocytosis, and thalassemia, an important complication of parvovirus B19 is a transient aplastic crisis. That’s because they already have fewer circulating red blood cells, so the breakdown of erythropoiesis causes severe anemia with symptoms like pale skin, fatigue, weakness, and shortness of breath. In immunocompromised clients, such as organ transplant recipients or those with HIV, the parvovirus can cause pure red blood cell aplasia. This is a form of severe anemia that develops because their weakened immune system cannot restrain the infection.
Now, the virus can be transmitted transplacentally, which can cause fetal anemia, miscarriage, and intrauterine fetal death. It can also cause nonimmune hydrops fetalis, which refers to the abnormal accumulation of fluid in soft tissues, which is often fatal. After the birth, the newborn may have respiratory problems from pleural effusion, heart problems from pericardial effusion, hepatosplenomegaly, and anemia.
Clinical manifestations of erythema infectiosum are usually absent and the client remains asymptomatic. But, on some occasions, after an incubation period of 4 to 14 days, or sometimes even 20 days, flu-like signs and symptoms may show up, including low-grade fever, malaise, muscle pain, headache, vomiting, diarrhea, and runny nose. Typically, just as the symptoms start to improve, a rash appears as uniform redness of both cheeks, sparing the area around the mouth, and giving the classic “slapped cheek” appearance, often called "slapped‑cheeks” rash. There can also be a maculopapular, lacy rash on the extremities and trunk, but sparing hands and soles of the feet. These usually last for a week or more, and then start fading, but may reappear if the skin is irritated, like when exposed to the sun, heat, cold, friction, or while exercising. In adults, the rash is less common, but if it develops, it’s often itchy. In contrast, adults more commonly develop arthralgia or joint pain, which affects small joints of the hands, wrists, feet, ankles, and knees, and is often symmetrical. The joints are not damaged by the virus, and the pain usually resolves within 3 weeks. It’s important to note that once the rash appears, shedding of the virus stops, so the client cannot spread the virus to others.
Now, diagnosis of erythema infectiosum is typically based on the client’s history and physical examination, followed by serological blood tests to detect parvovirus specific IgM antibodies. Serological blood tests are important to spot clients at high risk for complications, so it’s most commonly done in prenatal testing due to the risk of congenital abnormalities. Additionally, a PCR test can be used to detect viral DNA in maternal or fetal blood.
There’s no cure for erythema infectiosum, so the treatment is based on supportive care that includes rest and hydration, as well as medications, such as acetaminophen and NSAIDs to reduce fever, pain, and inflammation. Starch or oatmeal baths, and antihistamines may help reduce the itchiness of the rash. In the case of aplastic crisis, clients may need red blood cell transfusions, while severe fetal anemia may require intrauterine blood transfusion. This is where blood is administered directly into the fetus via the umbilical vein or artery. Finally, immunocompromised clients may receive intravenous immunoglobulin, or IVIG therapy, which involves giving them IgG antibodies from a donor blood plasma.
Alright, let’s take a look at the nursing care you’ll provide to a pediatric client with erythema infectiosum. Your primary nursing goal is to manage your client’s symptoms.
Sources
- "Wong’s nursing care of infants and children (12th ed.) ISBN: 978-0-323-77670-7 " Elsevier (2024)
- "Nelson textbook of pediatrics (21st ed.). ISBN: 978-0-323-52950-1 " Elsevier (2020)
- "Seidel’s guide to physical examination (10th ed). ISBN 9780323481953 " Elsevier (2023)
- "Essentials of Pediatric Nursing. 4th edition. ISBN: 978-1-975139-84-1 " LWW (2020)
- "Harrison’s principles of internal medicine. ISBN 978-1264268504 " Mcgraw Hill. (2022)
- " Advances in the Development of Antiviral Strategies against Parvovirus B19. 2019;11(7):659. " Viruses (Published 2019 Jul 18.)
- "Parvovirus B19 Infection. 379(24):2361." N Engl J Med. (2018)
- "A Meta-Analysis on the Seroprevalence of Parvovirus B19 among Patients with Sickle Cell Disease. 2019:2757450." Biomed Res Int. (Published 2019 Dec 9)
- "Mosby's diagnostic and laboratory test Reference (15th ed). ISBN: 978-0-323-67519-2 " Elsevier (2021)