Geriatric considerations - Gastrointestinal: Nursing
Geriatric considerations - Gastrointestinal: Nursing
Medical Surgical
Medical Surgical
Notes
| GERIATRIC CONSIDERATIONS - GASTROINTESTINAL | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
| MOUTH |
| |
| ESOPHAGUS |
| |
| STOMACH |
| |
| SMALL INTESTINE |
| |
| PANCREAS, LIVER, AND GALLBLADDER |
| |
| LARGE INTESTINE |
| |
| PATIENT AND FAMILY TEACHING |
| |
Transcript
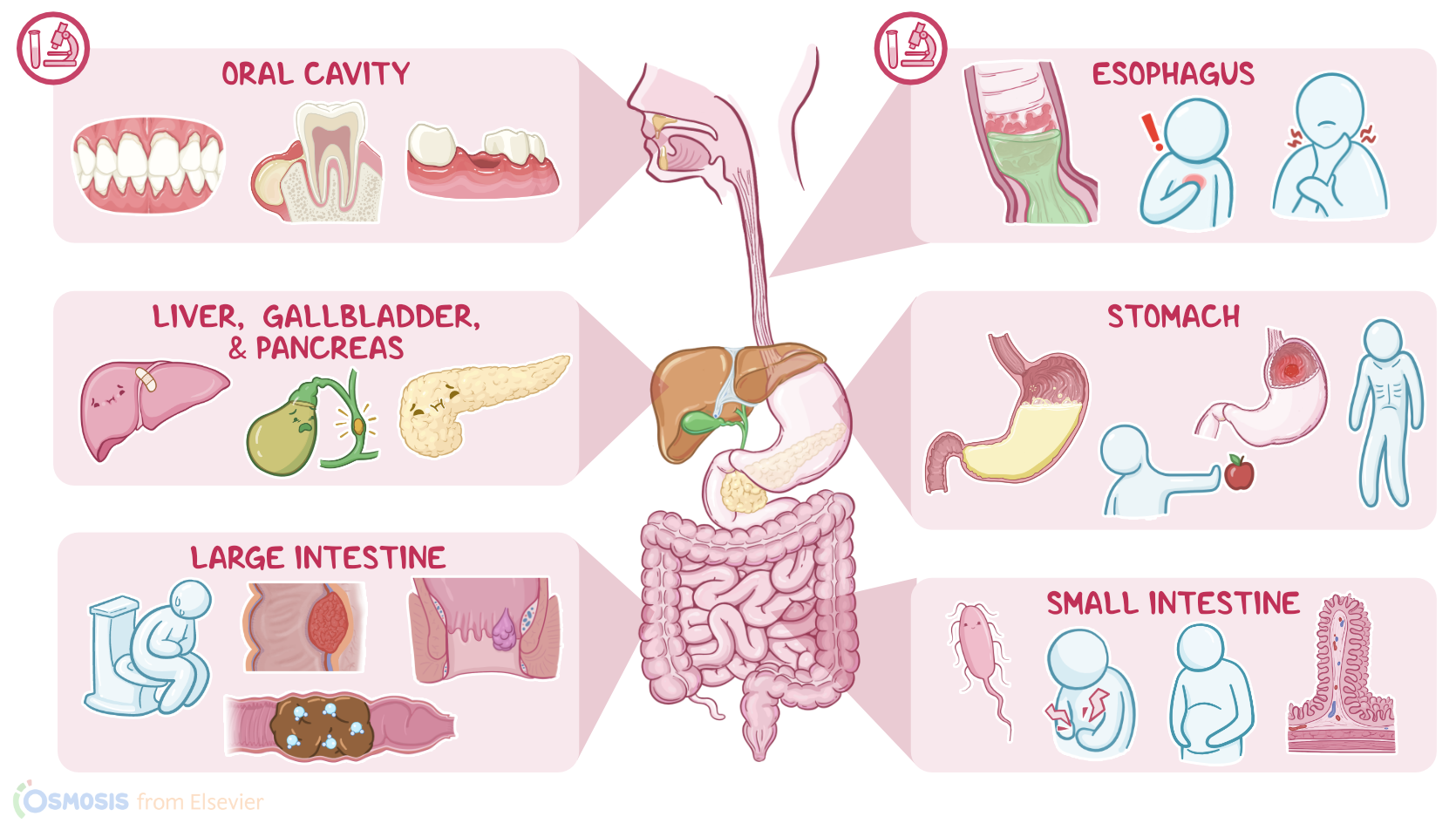
Geriatrics is the branch of medicine that deals with the physiology and psychology of aging, as well as the diagnosis and treatment of diseases affecting older clients. Now, aging affects various organ systems, one of which is the gastrointestinal system. All right, let’s start by reviewing the physiology of the gastrointestinal system, which is primarily responsible for mechanical and chemical digestion of food; absorption of nutrients; and finally, excretion of waste as feces. From top to bottom, the gastrointestinal tract starts with the oral cavity, then the esophagus, the stomach, the small intestine, the large intestine, and ends with the anus. First, let’s start with the oral cavity, which plays an important role in breaking down food. As a person ages taste buds atrophy and decrease in number, resulting in decreased ability to taste salty, sweet, bitter, sour and umami. This can decrease enjoyment of food, so poor eating habits and nutritional deficiencies could develop.
Many elderly clients also have periodontal disease, which refers to disease that affects the gum, or gingivae, and the underlying bones that support the teeth. The mildest form of periodontal disease is gingivitis, where just the gums are inflamed. If left untreated, gingivitis can progress to the more severe disease called periodontitis, where both gum and bones are affected and can eventually result in tooth loss. Additionally, with aging, the production of saliva by salivary glands decreases, which can lead to xerostomia or dry mouth, and this can also contribute to gingivitis and tooth decay. Elderly clients without teeth, or clients who have poorly fitting dentures, often find it hard to chew food. These clients tend to avoid certain hard to chew foods, which can eventually result in poor nutrition. Now, moving on to the esophagus, which is a part of the gastrointestinal system that propels the food from the pharynx down into the stomach. The esophagus and the stomach are separated by a muscular valve called the lower esophageal sphincter, which prevents the reflux of stomach contents back into the esophagus. Elderly clients may develop decreased esophageal motility, leading to symptoms such as dysphagia, as well as increasing the risk of aspiration.
Additionally, over time, the lower esophageal sphincter can lose tone, causing reflux of stomach content and causing gastroesophageal reflux disease, or GERD. The most common symptom is heartburn. Next, up is the stomach. The stomach produces gastric secretions that are made up of water; hydrochloric acid; as well as pepsin; mucus; and prostaglandins; but with aging, the amount of these gastric secretions decreases. Elderly clients can develop atrophic gastritis which can eventually lead to gastric acid hyposecretion, which results in malabsorption of nutrients such as vitamin B12, calcium, iron, zinc and folic acid. Less pepsin, which is an enzyme that chops up proteins, impairs protein digestion; and decreased mucus and prostaglandins makes the stomach more susceptible to the damage from gastric secretions. As a result, older clients have a higher risk of developing peptic ulcer disease. This is especially common in those who take aspirin or other nonsteroidal anti-inflammatory medications, such as ibuprofen.
Finally, gastric elasticity and motility decreases, leading to decreased gastric emptying time, which allows food to stay in the stomach longer. This may eventually reduce the client’s appetite and food intake leading to weight loss and nutritional deficiencies. Moving on to the small intestine, which is characterized by tiny ridges and grooves that are covered with little finger-like fibers called villi, that increase the surface area available for absorption of nutrients. Now, the intestinal surface is rich in enzymes, including lactase, maltase, and sucrase, which help digest sugars in the gastrointestinal lumen. There are also masses of lymphoid tissue called Peyer’s patches, which monitor the intestinal bacterial flora and prevent their overgrowth. Now, age-related atrophy of the intestinal villi decreases the available absorptive surface area, so less nutrients are absorbed. With aging, the production of lactase decreases, thereby increasing the risk of lactose intolerance. Additionally, there’s a reduction in the number of Peyer’s patches, which can result in the overgrowth of certain intestinal bacteria, leading to symptoms such as bloating and abdominal pain, as well as reduced absorption of calcium, iron, and folic acid. Okay, the absorption of nutrients in the small intestine is not possible without the help of the three accessory organs called the liver, gallbladder, and pancreas. The liver is the primary site of metabolism, protein synthesis, and bile production, which is stored and concentrated in the gallbladder. From here, the bile is squeezed into the small intestine where it serves as a fat emulsifier, meaning it helps break fats into smaller compounds that are easier to absorb.